Article Text

Statistics from Altmetric.com
In the year 2000, the European Society of Cardiology and the American College of Cardiology Committee jointly redefined myocardial infarction (MI) by an elevation of cardiac troponin T (cTnT) or I (cTnI) in conjunction with clinical evidence of myocardial ischaemia.1 Since then, cTnT and cTnI have replaced creatine kinase-MB (CK-MB) as the preferred biochemical markers for the diagnosis of MI. The decision for including cardiac troponins (cTn) in the diagnostic pathway was made because of the high sensitivity of cTn for detection of even small amounts of myocardial necrosis. An elevation of cTn indicates the presence of, but not the underlying reason for, myocardial injury. Hence, besides acute myocardial infarction (AMI), there is a myriad of potential diseases with troponin release, including acute pulmonary embolism, heart failure, myocarditis, and end stage renal disease. But regardless of what the release mechanism into the blood from cardiac myocytes is, elevated cTnT and cTnI almost always imply a poor prognosis. This article attempts to highlight the differential diagnosis of elevated cTn according to the various aetiologies of myocyte damage (table 1).
Causes of elevated troponins, prevalence, and underlying mechanism
WHAT ARE CARDIAC TROPONINS?
The troponin complex consists of three subunits—troponin C, troponin I, and troponin T—and is located on the myofibrillar thin (actin) filament of striated (skeletal and cardiac) muscle (fig 1). The cardiac isoforms troponin T and I are only expressed in cardiac muscle. Hence, cardiac troponin T (cTnT) and I (cTnI) are more specific than creatine kinase (CK) values for myocardial injury and, because of their high sensitivity, they may even be elevated when CK-MB concentrations are not. The cTn complex regulates excitation–contraction coupling in the heart. Cardiac troponin C (cTnC), a calcium (Ca2+) binding 18-kD-protein, regulates the activation of the actin filaments. cTnI (∼23 kD) inhibits contraction in the absence of Ca2+ binding to cTnC, and cTnT, the greatest subunit (∼35 kD), attaches the whole troponin complex to tropomyosin and to the actin filaments.2 cTn are found as structural (bound) proteins and as a small free pool that exists in the cytosol, which is about 6–8% for cTnT and 3.5% for cTnI. In some diseases, and supposedly in the case of pulmonary embolism or after ultra-endurance physical exercise, a transient leakage of the cytosolic pool of cTn, although never proven, cannot be excluded. Following myocardial damage, cTn egress rapidly from the myocyte and will appear in blood after 2–4 hours and persist long enough (up to 10–21 days) for convenient diagnosis. Furthermore, detection of cTn with immunoassays is easy, inexpensive, and the results are readily available, making them ideal biomarkers in most emergency facilities.

Schematic representation of the cardiac myofibrillar thin filament. Cardiac troponins exist in a structural (bound) form and in a free cytosolic pool. Cardiac troponins are released from myocytes as complexes or as free protein as indicated on the right.
CARDIAC TROPONINS IN ACUTE CORONARY SYNDROME (ACS)
Spontaneous acute myocardial infarction
In their current guidelines from 2000, the Joint European Society of Cardiology/American College of Cardiology committee redefined AMI as an elevation of cTn in blood above the 99th centile of a healthy reference population in conjunction with signs or symptoms of ischaemia.1 This did expand the diagnostic capacity to detect micro-MI which was not evident by CK-MB measurements. cTn do not only allow for more sensitive diagnosis of AMI but are also the most important predictor for acute thrombotic risk. Multiple randomised studies and several meta-analyses have substantiated the adverse prognostic risk associated with elevated cTn.3w1 For example, the meta-analysis by Ottani et al found that the odds ratio for death and MI was 3.44-fold at 30 days in the cTnT-positive group compared to patients with unstable angina.3 Further lowering of the cTn cut-off has been shown to improve risk stratification as pointed out in several randomised trials and registries.4 In addition, the implementation of a lower troponin cut-off as proposed by the guidelines led to a substantial increase in the frequency of MI diagnosis.w2
Several angiographic and angioscopic studies have demonstrated that the presence and magnitude of intracoronary thrombus is directly related to the concentration of cTn.w3 Therefore, cTn is regarded as a surrogate marker for active plaque and intracoronary thrombus. As an indirect finding, numerous randomised trials have found that patients with a positive troponin result benefit from a more intense antithrombin or antiplatelet treatment and also from an early invasive strategy.w4
AMI after percutaneous coronary intervention or open heart surgery
Percutaneous coronary intervention
In addition to spontaneous AMI, the current guidelines have also labelled post-procedural elevations of troponins after elective percutaneous coronary intervention (PCI) or coronary artery bypass graft surgery as AMI. However, minor elevations of cTn are frequently observed after elective PCI and are always found after open heart surgery. While there is no doubt as to the cardiac origin of troponins in these settings, neither the exact pathological mechanism nor the prognostic impact of these minor elevations are currently determined.
An elevation of cTn has been reported in 24–40% of patients after successful PCI in stable and unstable coronary artery disease.w5 w6 Possible reasons for the appearance of cTn include side branch occlusion, coronary dissection, bulky devices causing transient ischaemia, and microembolisms. Regardless of the exact mechanism, contrast-enhanced magnetic resonance imaging has demonstrated beyond doubt that postprocedural increases in cTn are related to myocardial necrosis.w7 In direct comparison, cTn were more sensitive for detection of minor injury and hence were detectable more frequently than CK or CK-MB after elective PCI. However, the relationship between the magnitude of CK-MB and future prognosis is seemingly more robust and consistent than the relationship of cTn with outcomes.w8 In a recent study involving 316 patients with stable symptoms, cTnI elevation following PCI correlated significantly with an increased risk of adverse events at 18 months.w5 In a study by Ricciardi et al, a threefold elevation of cTnI after successful elective PCI was predictive for future cardiac events, especially for early repeat vascularisation.5 In contrast, Cavallini et al showed that a cTnI elevation following coronary intervention was detected in 44.2% of the cases, but was not associated with a significant increase in long-term mortality.w8
Open heart surgery
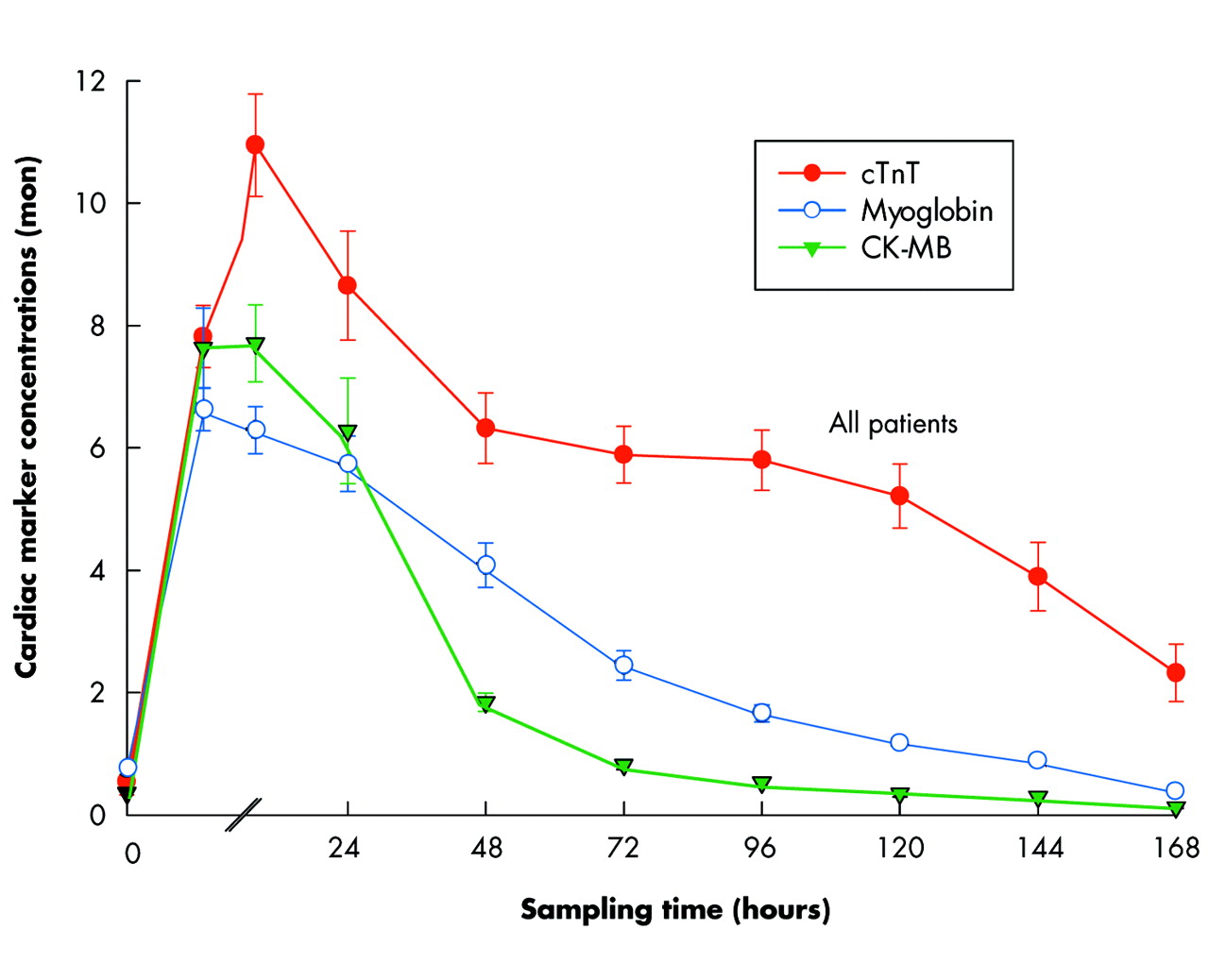
Cardiac troponins are always increased in small amounts and for an average time of five days following open heart surgery, even when no coronary artery bypass is effected.w9 Figure 2 shows the release curves of cardiac markers cTnT, myoglobin and CK-MB in 204 patients after open heart surgery. These troponin elevations do not necessarily reflect perioperative MI, but are more often attributable to myocardial cell injury resulting from incomplete cardioprotection, reperfusion injury, and direct surgical trauma. Hence, it is difficult to distinguish perioperative MI from these “normal” elevations of cTn, especially as no accepted cut-offs have yet been defined. Nevertheless, recent trials have established a significant association between elevated postoperative troponin values and increased mortality and morbidity.w10 Lehrke et al defined a cTnT concentration ⩾ 0.46 ng/ml 48 hours after open heart surgery as being predictive for long term mortality.6

Release curves of cardiac markers cTnT, myoglobin and CK-MB in 204 patients following open heart surgery. Concentrations are displayed as multiples of normal (mon). Cardiac markers are elevated up to seven days after open heart surgery.
Elevated troponin in suspected ACS without significant coronary artery disease
In symptomatic patients with suspected acute coronary syndrome (ACS) and even in those with elevated cTn, it is not uncommon that a significant culprit lesion is not detected by coronary angiography. It is tempting to speculate that a platelet-rich thrombus superimposed on the ruptured plaque has dissolved spontaneously or after antithrombotic treatment, or has dislodged leaving an insignificant atherosclerotic lesion at the time of angiography. Nevertheless, the presence of a troponin elevation implies a higher risk for death or AMI in these patients.7 Labelling of a positive troponin result as false positive in patients with a high suspicion of ACS is improper and misleading, possibly causing inadequate secondary prevention.
CARDIAC TROPONIN RELEASE UNRELATED TO ACS
Sepsis/septic shock and systemic inflammatory response syndrome
Among patients who are treated in intensive care units for sepsis or systemic inflammatory response syndrome (SIRS), elevated cTn have been detected in 36% (cTnT ⩾ 0.1 ng/ml) to 85% (cTnI > 0.1 ng/ml) of cases.8w11 This wide range of prevalence is mainly due to the different underlying causes of sepsis, the different troponin assays used, and the different cut-off values that were applied. In the majority of cases, significant coronary artery disease has been ruled out, indicating that other mechanisms underlie these troponin elevations. One reason for the release of cTn from damaged myocardial cells might be an oxygen supply–demand mismatch of the myocardium. As a consequence of fever and tachycardia the oxygen demand of the myocardium is increased. Simultaneously, oxygen supply of the myocardium is reduced due to systemic hypoxaemia from respiratory failure, microcirculatory dysfunction, hypotension and sometimes anaemia. In addition, local and circulating inflammatory markers including tumour necrosis factor α, interleukin 6 and reactive oxygen species, as well as bacterial endotoxins, may lead to direct myocardial injury by cytotoxic effects.w11 Moreover, elevated cTn values provide prognostic information and the extent of cTn elevation seems to correlate with the severity of the disease process. Ver Elst et al demonstrated that cTnI-positivity was strongly associated with LV-dysfunction (78% v 9% in cTnI-negative patients; p < 0.001). cTnI values were found to correlate significantly with the degree of hypotensionw12 and APACHE II score.w11 Finally, in a study by Spies and colleagues on 26 patients with sepsis, the group of patients with cTnT values ⩾ 0.2 μ/l had an increased mortality rate (83% v 38%, p = 0.02) compared to the group with cTnT values below this value.8
Pulmonary embolism
In acute pulmonary embolism (PE) elevated cTn are found in up to 50% of cases. For cTnT, rates of 32% and 50% were reported depending on the cut-off used (0.1 ng/ml v 0.01 ng/ml, respectively).9 w13 Among 38 patients with PE, elevated cTnI values (> 0.4 ng/ml) were seen in 47%.w14 Unfortunately, the reasons why cTn appear in blood after PE remain unclear. It is believed that cTn are released from injured right ventricular myocardial cells due to the acute dilatation of the right ventricle as a consequence of the abrupt increase of pulmonary artery pressure. Other possible reasons include reduced coronary perfusion, hypoxaemia from perfusion–ventilation mismatch, systemic hypoperfusion, or a combination of these factors. Studies investigating the release kinetics of cTnT in patients with PE showed that the peak cTnT was lower and persisted for a shorter time compared to cTnT values in AMI.10 Hence, in contrast to ACS, where cTn are released only after irreversible myocardial damage,11 in patients with PE, the brief appearance of small amounts of cTn suggests that troponin elevation may be caused by the efflux of the free cytosolic pool of cTnT due to transient membrane leakage.10 Figure 3 shows the differences in the kinetics of cTnT and N-terminal pro-B type natriuretic peptide (NT-proBNP) in two patients with acute pulmonary embolism who received thrombolysis or conservative treatment with standard heparin to resolve pulmonary hypertension.

{kind=link}
{kind=link}
{kind=link}
Time course of cardiac troponin T (cTnT) and N-terminal pro-brain natriuretic peptide (NT-proBNP) in two patients with acute pulmonary embolism. Patient A was treated successfully with thrombolysis and exhibited a rapid decrease of both biomarkers (cTnT: blue open circles; NT-proBNP: red solid circles) to normal values within 48 hours. Patient B received conservative treatment with standard heparin and showed an uncomplicated in-hospital course. Note the slower decline of both biomarkers.
Recently, cTn have emerged as important prognostic tools for risk stratification of patients with PE. Giannitsis et al showed that troponin-positive patients (⩾ 0.1 ng/ml) were at increased risk for a complicated in-hospital course including death, prolonged hypotension, cardiogenic shock, and need for resuscitation.9 Elevated admission cTnT values correlate significantly with severity of PE according to the grading system of Goldhaber (p = 0.003, r = 0.502, unpublished data) and values above 0.07 ng/ml predict all-cause mortality (3.7%).w15 Conversely, normal troponin values are associated with a good outcome. In several studies, the negative predictive value of normal troponins was determined at between 97–100%.9w13 Especially in patients with moderate PE, defined by haemodynamic stability and right ventricular dysfunction, elevated cTn may help in guiding therapeutic management. It has been shown that patients with right ventricular dysfunction determined by echocardiography are at increased risk of adverse clinical outcome.w16 This risk is 10-fold higher in the presence of elevated cTn (> 0.04 ng/ml) justifying a more aggressive treatment approach such as thrombolysis or embolectomy.w17
Acute and chronic heart failure
Briefly, elevated cTn in heart failure (HF) are associated with decreased left ventricular ejection fraction and correlate with severity of heart failure and prognosis. The aggravation of HF, ischaemic or non-ischemic, results from progressive myocyte loss caused by necrosis and apoptosis.w18 Additional factors, including the activation of renin–angiotensin–aldosterone and sympathic nervous systems as well as inflammatory mediators, may contribute to myocardial injury. Lost myocytes are replaced by fibrotic tissue leading to progressive cardiac dysfunction. cTn elevations in patients with HF reflect myocardial injury. In the setting of decompensated HF, the release of cTn is thought to be caused by excessive myocardial wall tension from acute volume and pressure overload. In addition, increased wall strain leads to subendocardial ischaemia. In patients with chronic stable HF, elevated cTnI values were found in 15–23% of cases (> 0.1 ng/ml).w19 w20 For cTnT, values above 0.1 ng/ml were reported in 10–15% of cases.12w21 There was no difference between the ischaemic and non-ischaemic group.12 w19 Of the patients admitted to hospital because of acute HF, 52–55% had elevated cTnT values.w21 w22 The presence of cTn in HF predicts a poorer short and long term outcome. Patients with increased troponin values have significantly lower ejection fractions, higher clinical grading of HF (New York Heart Association functional class), and greater mortality (hazard ratio 6.86).13 w23 Moreover, serial measurements of cTn could provide additional prognostic information.w21 A decrease of cTn is associated with an improvement of left ventricular function while persistently elevated or rising troponin values were observed in patients who eventually died.w23
Strenuous exercise
Several studies have reported the appearance of cTnT or cTnI after strenuous ultra-endurance exercise.14 w24 w25 However, neither the mechanisms nor the prognostic significance of elevated cTn are clear. Interestingly, following prolonged endurance exercise, only transient elevations of small amounts of cTn that decreased or normalised within 24 hours after the race have been detected.14 These changes in plasma concentrations are very different from those found in MI. This led to the assumption that elevated cTn could result from a transient release of the cytoplasmatic pool of cTnT and cTnI and not from continuous release of structurally bound troponin after myocardial necrosis. On the other hand, autopsy findings and extensive cardiac examinations have revealed critical coronary heart disease or significant structural heart disease in presumably healthy athletes.w26 w27 Hence, elevated cTn could result from underlying subclinical heart disease being unmasked by strenuous exercise. In a recent study on 10 well-trained healthy athletes, who participated in an ultra-marathon of 216 km in Death Valley at extreme environmental conditions, we found that cTnT values remained below detection limits during and after the run, even in one athlete who developed severe exercise-induced rhabdomyolysis with a CK value of > 27 000 U/l (unpublished data). Further information is needed to clarify some inconsistencies in this field.
Acute pericarditis/myocarditis
In addition to AMI and acute pulmonary embolism, acute pericarditis/myocarditis is commonly diagnosed in patients with elevated troponins presenting to the emergency room with acute chest pain. Although troponins are not present in the pericardium, cTnI was reported to be elevated in 32–49% of cases of pericarditis,w28 w29 as a consequence of the involvement of the epicardium in the inflammatory process. In patients with acute myocarditis cTnI concentrations have been found to be increased in 34% of patients.w30
Usually in patients with suspected pericarditis, coronary angiography is performed to rule out MI. In the absence of significant coronary disease, endomyocardial biopsies (EMB) are taken to establish the diagnosis. However, in only 10–25% of patients with clinically suspected myocarditis have EMB shown the typical myocytolysis and lymphocytic infiltrates.w31 Elevated cTnT values are seemingly more sensitive than EBM and may confirm the clinical suspicion of myocarditis, even in the absence of histological signs of myocarditis.w30 w31
Cardiotoxic chemotherapy
Most chemotherapeutic agents, including anthracyclines, alkylating agents, anti-metabolites or anti-microtubules, can have cardiotoxic side effects. Observed adverse cardiac events following chemotherapy are ischaemia (anti-metabolites, alkylating agents), endomyocardial fibrosis and cardiomyopathy (alkylating agents—for example, anthracyclines), pericarditis (alkylating agents—for example, cyclophosphamide), and different types of arrhythmias (anti-microtubules—for example, paclitaxel).w32 Routinely, cardiac toxicity is detected by echocardiography, ECG, or endomyocardial biopsies. Recent data suggest that biochemical markers such as troponins and natriuretic peptides could be useful in identifying patients at risk for myocardial damage and in monitoring the development of cardiac damage.w33 w34 However, their role in predicting clinical and subclinical myocardial damage and in influencing therapeutic strategies remains to be evaluated by future clinical trials.
High frequency ablation/external current cardioversion/defibrillator shocks
Following radiofrequency catheter ablation, an elevation of cTn has been reported in more than 90% of patients and is related to direct traumatic myocardial injury,w35 but these elevations have no prognostic significance. External current cardioversion (ECV) of atrial fibrillation or flutter caused no or only small increases of cTnIw36 and no increases of cTnT,w37 especially when biphasic modus was used.w36 Repetitive defibrillator shocks because of ventricular tachycardia or fibrillation or mechanical cardiac resuscitation are known to release cTn. These elevations seem to indicate the diagnosis of AMI presenting with life-threatening arrhythmias rather than myocardial damage caused by ECV.w38
Cardiac infiltrative disorders
In systemic amyloidosis, the extent of cardiac involvement is tightly linked to the clinical outcome. In one retrospective analysis on 261 patients with systemic amyloidosis, Dispenzieri and colleagues showed that the median survival of patients with detectable cTnI and cTnT was significantly reduced (six and eight months, respectively) compared to that of patients with normal values (22 and 21 months, respectively).w39 It is believed that extracellular amyloid deposition causes compression of myocytes with subsequent release of cTn. In many patients, the diagnosis of cardiac involvement is made incidentally by a positive troponin result in the absence of signs or symptoms of ACS. Therefore, it is tempting to speculate that at least in patients with a systemic disease with potential involvement of the heart, routine measurement of cardiac troponin could allow earlier detection of prognostically adverse cardiac involvement.
Post-heart transplantation
Since the early 1990s it has been known that cTn can be elevated in nearly all heart transplant recipients for up to three months after successful transplantation.w40 w41 In the following years, cTn were found to be related to allograft rejection. In 1998 Dengler and colleagues found that cTnT values increased in parallel with the severity of graft rejection according to the ISHLT (International Society of Heart and Lung Transplantation) grading system. In the group with severe rejection (ISHLT grade 3 and 4), nearly all patients had elevated cTnT values; if cTnT was negative, significant rejection could be excluded with a probability of 96.2%.15 Moreover, in a study on 110 heart transplant recipients, Labarrere et al showed that cTnI was elevated in all patients during the first month following heart transplantation; however, only those with persistently elevated cTnI values during the follow-up period of 12 months were at increased risk for subsequent development of coronary artery disease and graft failure.w41 Today, endomyocardial biopsies are the gold standard for diagnosis of allograft rejection. Cardiac troponins can provide additional information, especially if they are negative.
Myocardial contusion
In the setting of severe blunt chest trauma, cardiac contusion occurs in 3–56% of cases. Because cardiac contusion may cause lethal arrhythmias and heart failure, diagnosis is of great importance. Cardiac troponins have been reported to be elevated in 15–45% of patients with cardiac contusion.w42 w43 Their high negative predictive value (between 21–94%) helps in precluding cardiac injury after severe chest traumaw44 in conjunction with standard echocardiography.
RENAL FAILURE/END STAGE RENAL DISEASE
Troponins in symptomatic patients with suspected ACS
In symptomatic patients with suspected ACS, elevation of cTn is associated with adverse outcomes regardless of the degree of renal insufficiency.4 However, in patients with advanced renal failure, cTn concentrations develop higher peaks and troponin remains detectable for longer periods. Given that patients with end stage renal disease (ESRD) already have elevated troponin values before the acute cardiac event, repeated early measurements are needed to detect a pronounced rise indicating an acute ischaemia. Unfortunately, there are no approved protocols on the frequency and intervals of blood sampling.
Troponins in asymptomatic patients without suspicion of ACS
In asymptomatic patients with ESRD interpretation of elevated troponin values is much more difficult. Cardiovascular disease is by far the leading cause of death in patients with ESRD, hence a clinically silent cardiac pathology can always underlie these troponin elevations. Most studies on prevalence and prognostic impact of cTn in patients with ESRD were conducted in patients with haemodialysis as renal replacement therapy. Only sparse information exists for peritoneal dialysis patients. Both cTnT and cTnI are commonly increased in asymptomatic patients with ESRD, even when there is no suspected myocardial ischaemia. Using third generation assay for cTnT, up to 53% (10% coefficient of variation, > 0.03 ng/ml) of haemodialysis patients had elevated cTnT values,16 w45 w46 while elevation of cTnI was less frequently observed (up to 19%).w47–49 This finding led to the assumption that cTnI would be a more specific marker for myocardial ischaemia in patients with ESRD than cTnT. This is not true, however, and there are some possible explanations for the different prevalence of the two troponins. First, as mentioned above, the cytosolic unbound fraction of cTnI is half of that of cTnT (approximately 3.5% v 7%). Secondly, the cTnI molecule is more positively loaded than cTnT and has a higher affinity for the negative loaded dialysis membrane.17 Thirdly, cTnI is only released in complex with cTnC, so that epitopes necessary for the antibody binding in the immunoassay could be covered.w50 Finally, the cTnI protein is more unstable than cTnT and might therefore undergo fragmentation, oxidation and phosphorylation which might influence epitope binding.w51
Why do cTn appear in blood in patients with ESRD?
The answer to this question has been sought but no satisfying explanation has been found yet. Several hypotheses have been discussed. First, a re-expression of cTn in uraemic myopathic skeletal muscle was assumed. In 1997, McLaurin and colleagues reported expression of cTnT, but not cTnI, in four of five skeletal muscle biopsies of haemodialysis patients.w52 In several subsequent studies, re-expression of cardiac isoforms in skeletal muscle could be convincingly excluded.18 w53
Secondly, reduced renal clearance of cTn in ESRD patients was widely believed to contribute to elevated cTn values.
In addition, increased cTn values can be caused by concomitant diseases known to be associated with cTn release such as severe HF, left ventricular hypertrophy leading to a subendocardial ischaemiaw54 or renal anaemia with consecutive oxygen supply–demand mismatch.
Recent evidence suggests that cTnI is fragmented into pieces of 8–25 kD that are normally released in very small quantities in the blood and are sufficiently small enough to be cleared by the healthy kidney.w55 In patients with ESRD, these microfragments cannot be cleared from blood and are detectable by immunoassays.
Are troponin-positive patients with ESRD at increased risk for death?
Several large observational studies have clearly shown that elevated concentrations of cTnT in patients with ESRD are valuable, independent, short and long term predictors of cardiac death.16,19 w45 In a prospective study by Apple et al on 733 patients with chronic intermittent haemodialysis, the two year mortality rate rose with increasing cTnT, reaching 47% for cTnT ⩾ 0.1 ng/ml. The adjusted relative risk of death for elevated cTnT (> 99th centile) was 3.9 (confidence interval 1.9 to 7.9; p < 0.001). In direct comparison, the prevalence of a positive troponin I result across all cut points was much lower than the prevalence of cTnT. In addition, cTnI failed to predict outcomes in patients with ESRD. Accordingly, the US Food and Drug Administration has only recommended the use of cTnT for risk stratification in ESRD patients.
Do false-positive troponin results exist?
By definition, 1% of healthy volunteers with minor elevation of cTnT must be labelled false positive because only 99% of tested healthy volunteers had cTnT values below the lower limit of detection (99th centile). In clinical practice, an elevation of cTn is more often misinterpreted as false-positive when significant coronary artery disease has been ruled out by coronary angiography in a symptomatic or asymptomatic patient. This labelling is inappropriate and frequently leads to cessation of further diagnostic work-up or adequate treatment. Usually, cTn confirms and supports a clinical suspicion or diagnosis. The usefulness of troponin largely depends on the quality of the clinical judgement and the level of clinical probability.
In patients with a high probability of ACS, absence of a significant lesion does not contradict the presence of an unstable plaque. In patients with low or intermediate probability of ACS other differential diagnoses should be considered. Thus, frequently cTn is the only indicator of cardiac pathology in numerous cardiac diseases or systemic diseases with cardiac involvement. Elevated troponins could therefore open an avenue for more precise or specific diagnostic procedures.
The term false positive troponin should be restricted to analytical issues. A summary of potential reasons is given in table 2. The continuous improvement of assay performance has reduced rates of analyte-related false positive results over the years by eliminating heparin interference, or cross-reactivity with skeletal muscle. For example, first and second generation troponin assays often yielded positive results in patients with severe skeletal muscle injury because of an unspecific binding of skeletal muscle troponin T to the test tube.20 Using a third generation cTnT assay, in a recent study on 10 ultra-marathon athletes, we found no cross-reactivity between cTnT and CK, neither in exercise-induced skeletal muscle trauma nor after rhabdomyolysis (unpublished data).
Analytical causes of false-positive troponins
Additional references appear on the Heart website—http://www.heartjnl.com/supplemental
REFERENCES
Supplementary materials
Files in this Data Supplement:
- view PDF - Web-only references.
Footnotes
-
In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article
Linked Articles
- Miscellanea
- Miscellanea
- Miscellanea
- Miscellanea
- Miscellanea