Article Text

Statistics from Altmetric.com
Pulmonary stenosis (PS) accounts for approximately 8% of all congenital heart defects.1 Valvular PS is usually an isolated defect, but it can be associated with other congenital heart defects, such as atrial septal defect (ASD), ventricular septal defect (VSD), and persistent ductus arteriosus. Combined valvular and infundibular PS can be part of tetralogy of Fallot (ToF).
The clinical presentation of PS may vary from critical stenosis in the newborn, to asymptomatic mild stenosis without need for therapy throughout life. The need for treatment of critical PS in the newborn is obvious, but the optimal timing, type of treatment, and follow-up strategy for the asymptomatic patient is less well defined.
Epidemiology
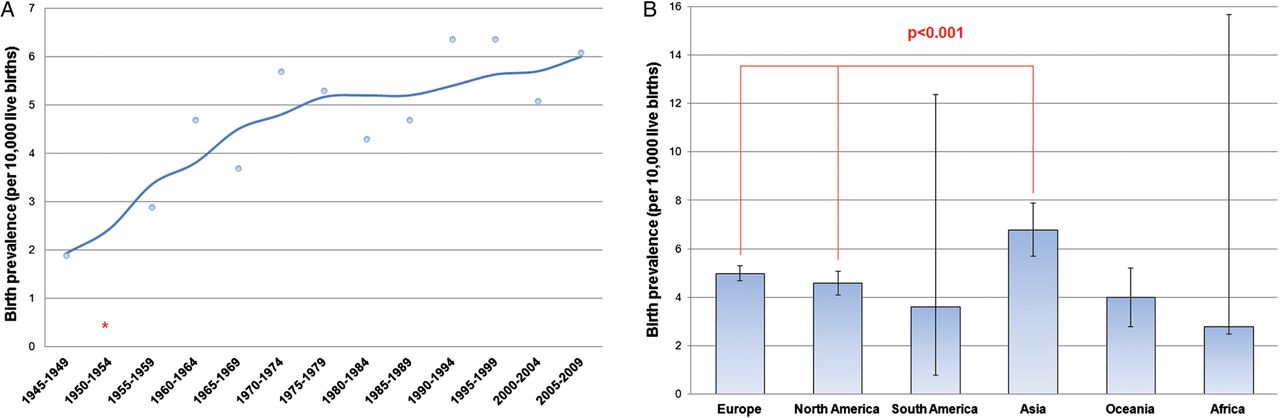
PS occurs in about 1 per 2000 live births worldwide.1 The prevalence seems to be steadily increasing over time (figure 1A). There is a slightly higher birth prevalence in Asia as compared to Europe and the USA1 (figure 1B). The underlying cause is not well known, but should be sought in genetic, environmental, and dietary factors. There is increasing evidence that epigenetic modifications play an important role in certain diseases apart from genetics, and this might also be true for PS.w1 w2 Since an increasing number of patients had surgical or interventional repair during childhood, more and more adults will be seen with long term residual lesions like pulmonary regurgitation (PR) and restenosis.

Birth prevalence of pulmonary stenosis. (A) Time course of birth prevalence until 2010. (B) Reported birth prevalence per continent. Adapted with permission from van der Linde et al.1
Morphologic classification and aetiology
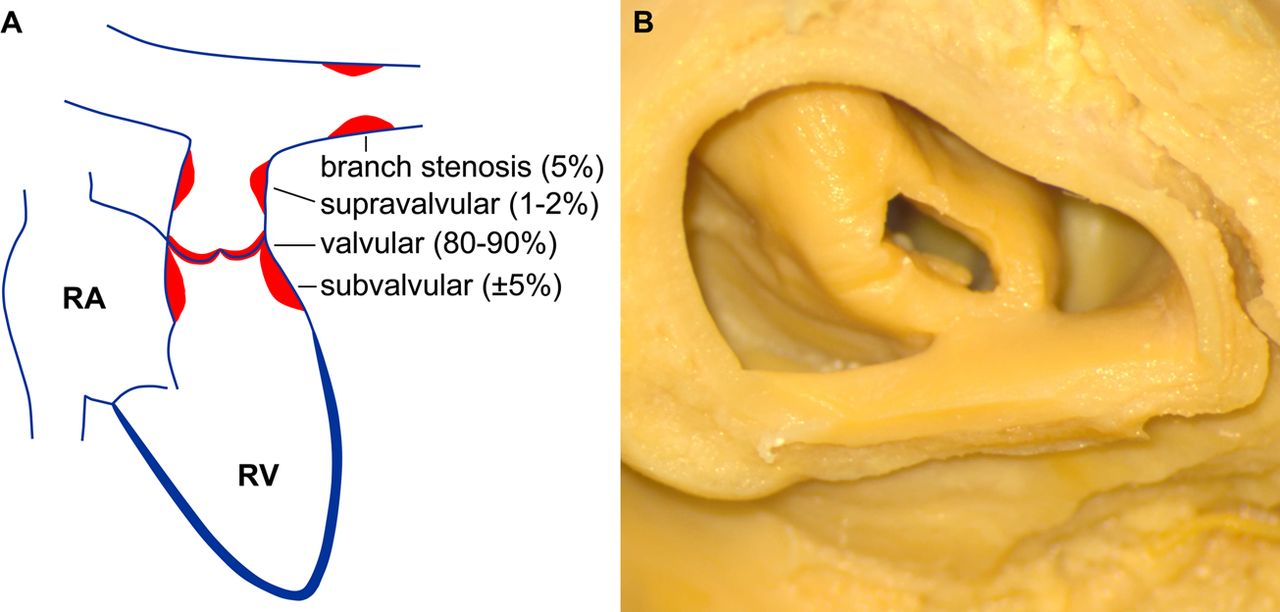
PS can be valvular, subvalvular (infundibular) or supravalvular (figure 2A). Valvular stenosis is by far the most common form.
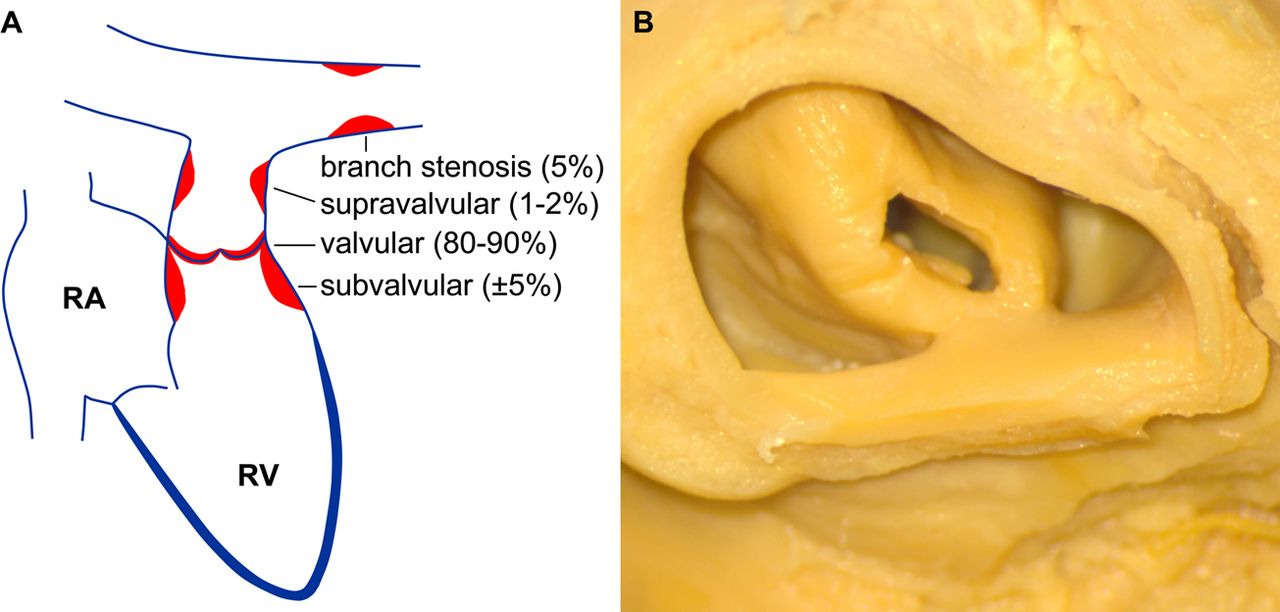
Morphology of pulmonary stenosis (PS). (A) Schematic representation of different types of PS. RA, right atrium; RV, right ventricle. (B) Doming pulmonary valve. Courtesy of Dr MM Bartelings and Dr MRM Jongbloed, Department of Anatomy & Embryology, Leiden University Medical Centre, the Netherlands.
Valvular PS
In valvular PS, the pulmonary valve usually has a dome-like shape with a narrow central opening (figure 2B). Rudimentary raphes can be seen. Less often, the valve is dysplastic, with myxomatous thickened leaflets. The latter is associated with Noonan syndrome (table 1). In ToF there often is a stenotic bicuspid or unicuspid pulmonary valve. Valvular PS can also be associated with other congenital heart defects such as ASD, Ebstein's anomaly, double outlet right ventricle, and transposition of the great arteries.
Common genetic syndromes associated with pulmonary stenosis
Subvalvular PS
Subvalvular PS can be infundibular or subinfundibular. Infundibular PS is usually seen as part of ToF, while isolated infundibular PS is very rare. Secondary infundibular hypertrophy may occur in valvular PS: because the right ventricular (RV) outflow tract (infundibulum) is a circular muscular structure, reactive RV hypertrophy can cause a dynamic outflow obstruction. Subinfundibular PS is also known as ‘double chambered right ventricle’ (DCRV). In that case, the RV cavity is divided into a high pressure inlet part and a low pressure outlet part, by anomalous muscle bundles. This can be either a hypertrophied moderator band or local hypertrophy that may develop as the consequence of a high velocity jet of a small VSD, directed at the opposing RV wall. A DCRV can be misinterpreted as RV hypertrophy due to, for example, pulmonary hypertension. In contrast to most other causes of right ventricular outflow tract (RVOT) obstruction, a DCRV can be progressive in adult life.
Supravalvular PS
Supravalvular PS can be isolated, but is often associated with other cardiac or extracardiac abnormalities. It is described in several syndromes, including Williams–Beuren, Noonan, Allagile, DiGeorge, and Leopard syndrome (table 1). Furthermore, it can occur in the clinical picture of congenital rubella syndrome. The stenosis can be located in the common pulmonary trunk, the bifurcation or the pulmonary branches.
Clinical presentation
In the newborn with a critical PS, the suprasystemic RV pressure may result in RV dilatation and failure with severe tricuspid regurgitation (TR) and cyanosis due to right-to-left shunting over the foramen ovale or an ASD. These infants may present in heart failure and will often be duct dependent. However, most patients with mild to moderate PS are asymptomatic and will be discovered by a murmur during routine physical examination in infancy or childhood. There can be mild exertional dyspnoea and fatigue. In untreated severe PS, the inability to increase pulmonary blood flow during exercise can lead to chest pain or syncope.
Diagnostic tools
ECG
In patients with mild PS the ECG can be normal, perhaps showing only a more pronounced right-ward axis deviation. In children and adolescents a right axis up to −100° to −110° can be completely normal.w3 However, in more severe stenosis, RV hypertrophy, further rightward axis deviation, high R wave amplitude in lead V1 and deep S waves in the left precordial leads, with an R:S ratio <1 in V6, can be seen.w4
Echocardiography
Transthoracic two dimensional (2D) echocardiography and Doppler imaging is the clinical standard to detect PS and quantify its severity. For visualisation of the pulmonary valve, the parasternal short axis view and alternatively the anterior angulated subcostal or subxyphoid view are used (figure 3). These latter views are very useful in neonates and children, in whom the distances are small. Furthermore, in adults it is sometimes possible to obtain a parasternal long axis image by rotation of the probe by 90° and angulating towards the right shoulder.

Echocardiographic and angiographic images of pulmonary stenosis (PS). (A) Two dimensional parasternal short axis view of a doming pulmonary valve. (B) Corresponding Doppler image showing moderate PS. (C) Cineangiographic frame showing doming of the pulmonary valve and hyperkinetic contraction of the infundibular myocardium. (D) Cine-radiographic frame showing balloon dilatation of the stenotic pulmonary valve. Note the ‘waisting’ of the balloon at the site of stenosis.
In the parasternal short axis view, a thickened and often dome shaped pulmonary valve can be seen (figure 3A). Peak and mean gradients can be measured by Doppler imaging. The orientation of the RVOT in the chest and the posterior direction of the pulmonary artery make it relatively easy to align the echo beam to the pulmonary flow, so off-angle interrogation is not a real problem in valvular and supravalvular stenosis. Continuous wave Doppler imaging can best be obtained with the sample volume located just distally to the tips of the pulmonary valve. Pulsed wave Doppler is useful to discriminate between subvalvular, valvular and supravalvular stenosis. In DCRV, however, alignment problems can be an issue, making it difficult to measure the true gradient. Double checking with RV systolic pressure estimates from the TR gradient will prevent underestimation of the true gradient. Both in multilevel stenosis and more than mild regurgitation, the modified Bernouilly equation will overestimate the real gradient. Here too, the TR gradient will give a better estimate of the true gradient. PS is graded as mild, moderate or severe (figure 4).2

Severity grading of pulmonary stenosis.
Accompanying PR can be visualised with colour Doppler and continuous wave Doppler techniques. PR severity can be estimated by the jet length and width compared to the annular diameter and RVOT on colour Doppler imaging. This is sometimes difficult to assess, especially in eccentric PR. Diastolic retrograde flow in the pulmonary artery branches, however, is always a sign of severe PR. This should always be looked for in particular. A PR pressure half time <100 ms is also an indicator of haemodynamically significant PR. Semiquantitative assessment of PR by the PR index (ratio of PR duration to diastolic duration) can be useful.3 A PR index <0.77 yields 100% sensitivity and 85% specificity for identifying patients with a significant PR (ie, >24.5% regurgitation). In severe PR, RV diastolic function can become restrictive. Although this reflects abnormal haemodynamics, its effect is beneficial: the high end-diastolic RV pressure causes end-diastolic antegrade flow over the pulmonary valve and thereby limits the amount of PR.
Quantitative assessment of RV volume and function by 2D echocardiography is limited. Three dimensional (3D) echocardiography can accurately estimate RV volume and ejection fraction,4 w5 but it has limitations due to a limited acoustic window. Qualitative assessment is hampered by subjectivity, but can be used to estimate dilatation and deterioration of function over time. Routine work-up of the right heart includes parasternal long and short axis views for measurements of RV inflow and outflow dimensions (figure 5) and assessment of the tricuspid and pulmonary valve, and the apical four chamber view for long and short axis dimensions, tricuspid annular plane systolic excursion (TAPSE), and fractional area change.

Echocardiographic measurements of right ventricular dimensions. (A) Parasternal long axis view. (B) Parasternal short axis view. (C) Apical four chamber view. Ao, aorta; LA, left atrium; LV, left ventricle; PA, pulmonary artery; RA, right atrium; RV, right ventricle; RVIT, right ventricular inflow tract; RVLAX, right ventricular long axis; RVOT, right ventricular outflow tract.
MRI
MRI is useful for studying the anatomy of the RVOT, pulmonary artery and its branches, using cine and phase contrast techniques and 3D gadolinium imaging. The precise location of the stenosis can be visualised, which is valuable in distinguishing between subvalvular, valvular and supravalvular stenosis especially. Flow artefacts in gradient echo images can be indicative of stenosis or regurgitation. Velocity mapping, based on the principle of phase shift between stationary and moving tissue, which can be translated into voxel velocity at any point of the cardiac cycle, can be used to study the peak velocity of flow over the pulmonary valve. Because this technique detects the velocity of the fastest protons in the flow, the maximum velocity measured by MRI is often higher than that measured by echo Doppler, in which the mean velocity of many erythrocytes is calculated. A major drawback of velocity mapping MRI techniques is that the technique is based on laminar flow, and is detrimentally affected by turbulent flow patterns such as in valvular stenosis. Consequently, for determination of flow velocities, echocardiography is the technique of choice. Flow volumes, however, can be accurately assessed by MRI. This is especially useful for determination of the regurgitant volume in PR after a prior intervention. MRI is considered the gold standard for assessment and quantification of (right) ventricular volume, mass and function. It is not bothered by the geometric assumptions that are unavoidable in echocardiography.
Limitations of cardiac MRI are its incompatibility with most pacemakers and other metal devices, the requirement of breath holds, and a regular heart rhythm. Furthermore, its availability is still limited and costs are high, and claustrophobia may make a patient unsuitable for MRI.
Multislice CT
Multislice CT (MSCT) might be the superior diagnostic technique to study the anatomy of the RVOT and the pulmonary arterial tree especially, but it lacks possibilities for volumetric and functional assessment. For routine follow-up, MRI is preferred over MSCT where possible, because of the ionising radiation of the latter, especially where young patients are concerned. Moreover, for image acquisition with MSCT, a low heart rate is required.
Cardiac catheterisation and angiography
This has been the classic way of determining the severity of PS. Pressure gradients can be measured directly and angiography represents anatomy accurately (figure 3). Nowadays, cardiac catheterisation is used for invasive treatment, because the diagnosis and severity of stenosis will already have been assessed by echocardiography. For comparison with the older literature, on which guidelines are still partly based, translating the Doppler derived peak instantaneous gradient into the peak-to-peak invasive gradient becomes relevant. Although overestimation of the gradient by Doppler is less likely to occur in pulmonary valve stenosis than in aortic stenosis, in case of doubt severity confirmation by invasive measurement is warranted.
Treatment
Indications
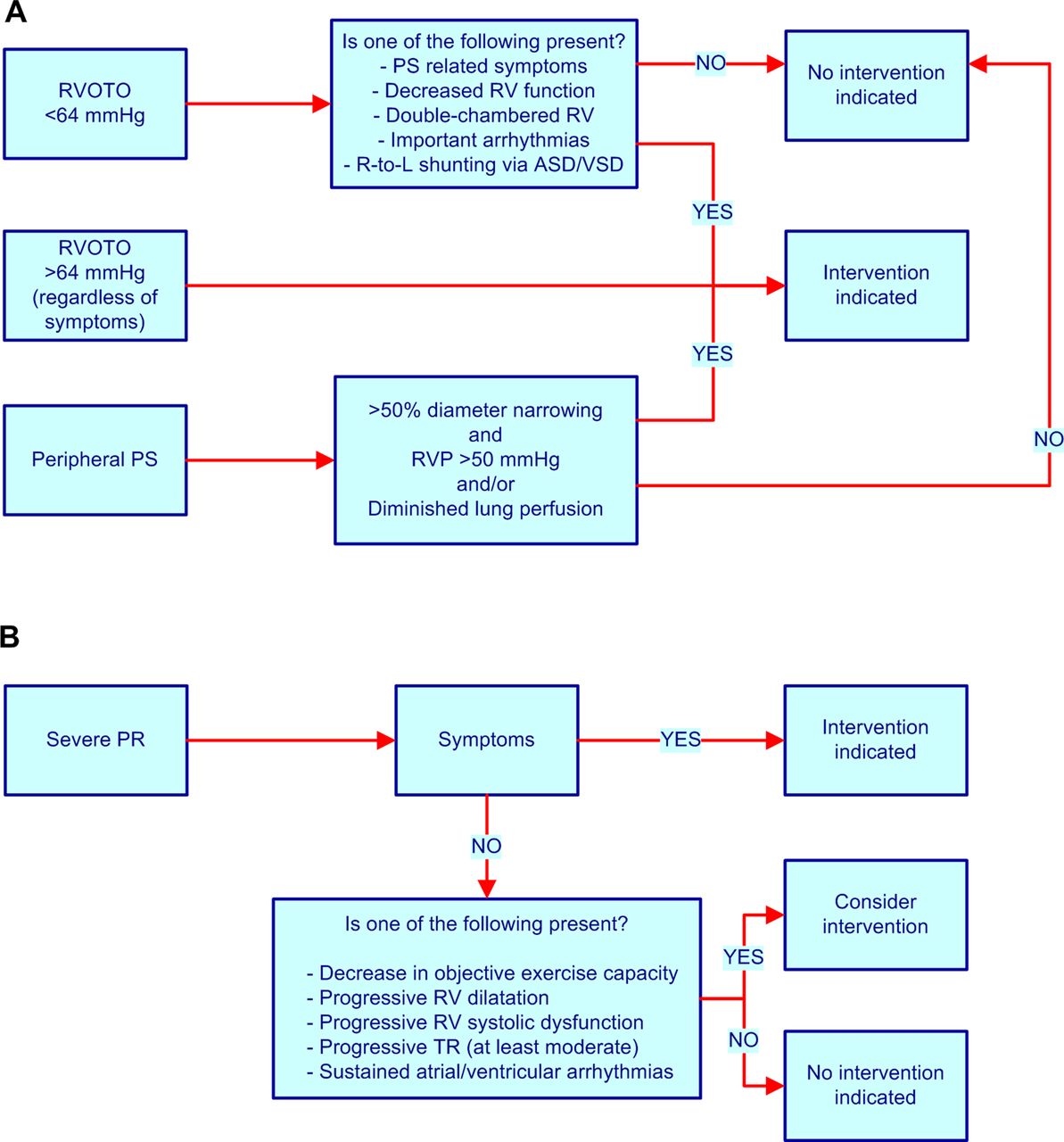
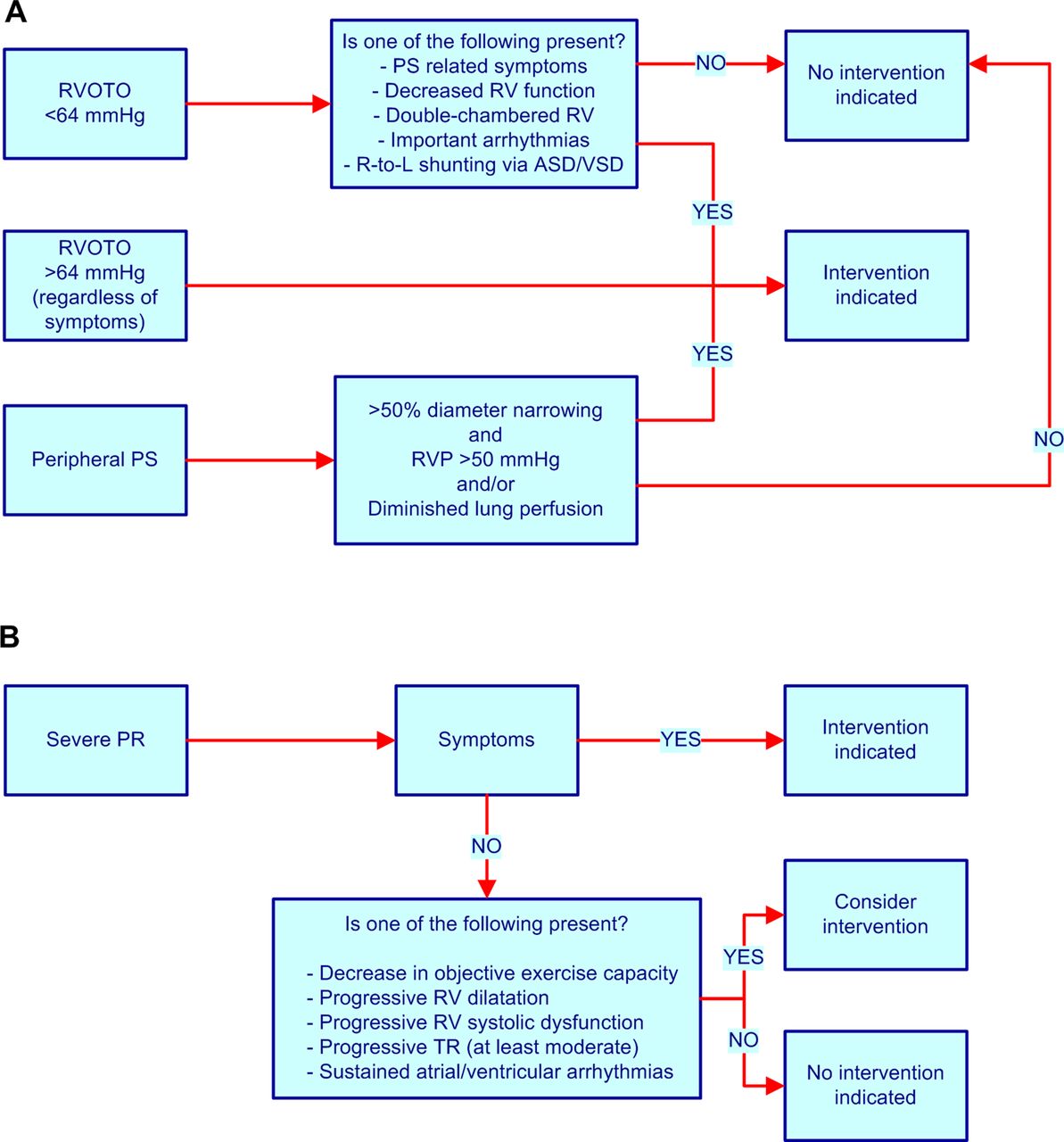
The goal of treatment is relief of the RVOT obstruction, thereby alleviating the pressure overloaded RV. Any obstruction in the RVOT and/or pulmonary valve with a Doppler derived peak instantaneous gradient >64 mm Hg (peak velocity >4 m/s) should be repaired. Indications for treatment in moderate PS or peripheral pulmonary artery stenosis are summarised in figure 6.5 In case of asymptomatic valvular stenosis in which balloon valvuloplasty is not possible, surgical repair should be performed in the presence of a systolic RV pressure >80 mm Hg (TR velocity >4.3 m/s).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Indications for intervention in pulmonary stenosis (A) and regurgitation after previous treatment (B). In asymptomatic patients in whom valve replacement is the only option, the threshold for intervention is higher: surgery should be performed in the presence of a systolic right ventricular pressure >80 mm Hg (tricuspid regurgitation velocity >4.3 m/s). ASD, atrial septal defect; PR, pulmonary regurgitation; PS, pulmonary stenosis; R-to-L, right-to-left; RV, right ventricle; RVOTO, right ventricular outflow tract obstruction; RVP, right ventricular systolic pressure; TR, tricuspid regurgitation; VSD, ventricular septal defect.
Choice of treatment
Since balloon pulmonary valvuloplasty (BPV) was introduced in the 1980s, it has rapidly replaced surgical valvotomy as the preferred treatment. If there is a hypoplastic pulmonary annulus or a severely dysplastic valve, or if the stenosis is infundibular or associated with other lesions which have to be repaired, the result may be limited and surgical treatment will often be necessary.
Balloon pulmonary valvuloplasty
Venous access is usually achieved via the femoral vein, but access through the jugular, axillar or hepatic veins is possible in the case of occluded femoral veins. The valve is dilated with a balloon sized 1.2–1.4 times the pulmonary annulus. The procedure is considered successful when the invasive gradient is reduced to <30 mm Hg. In experienced hands the risk of death or major complications is very low, 0.24% and 0.35%, respectively.w6 Complications, including transient bradycardia and hypotension during balloon inflation, transient or permanent right bundle branch block or atrioventricular block, balloon rupture, tricuspid papillary muscle rupture, and tears in the pulmonary artery have been reported, but all are rare. Development of post-procedural infundibular stenosis may occur, but this usually resolves over time. Rarely, β-blocker treatment is necessary for this dynamic RVOT obstruction after balloon valvulotomy.
Surgical repair
Many different approaches have been used to repair valvular PS. The initial surgical correction consisted of a closed valvulotomy, first performed in 1948 by Lord Brock. Afterwards the procedure evolved to open valvulotomy, initially using inflow occlusion and later on cardiopulmonary bypass. Nowadays, an open commissurotomy or valvulotomy is performed, in which the pulmonary trunk is opened through a vertical incision. If present, the fused commissures of the valve are opened by incision. Valvular tissue is excised only when other methods fail to achieve a wide opening. The same goes for the use of a transannular patch of autologous pericardium. In isolated valvular PS, the perioperative risk is very low, and the risk of death approaches zero.6 As initial treatment, valve replacement is rare.
Redo intervention and future options
In patients with significant residual PS after BPV, a redo BPV can be performed with a larger balloon. If this is still unsuccessful, surgical intervention will be necessary. Sometimes pulmonary valve replacement cannot be avoided. Then implantation of a non-mechanical valve is preferred, because the risk of thrombosis in pulmonary mechanical valves is higher than in mechanical valves in the aortic position. Our preference is implantation of a pulmonary homograft, but availability of homografts can be limited. Other surgeons might prefer the use of other bioprosthetic valves.
Surgical valve replacement may also be necessary in the case of severe, haemodynamically significant PR after BPV or previous surgery. In patients who have already received a non-mechanical valve, stenosis or regurgitation can develop over time. In those patients, percutaneous valve implantation may be an option. For PR after correction with a transannular patch, percutaneous intervention is not possible yet, but new devices are being developed. The first in-human implantation of a new, self expandable valve has been reported.7
Late outcome
Unoperated patients
The natural history of patients with mild PS is usually benign. In the Second Natural History study,8 patients with an invasive peak-to-peak gradient ≤25 mm Hg had normal survival and no progression of their stenosis in 25 years of follow-up; patients with a gradient between 25–49 mm Hg had a 20% chance of ever needing an intervention; and the majority of patients with a gradient ≥50 mm Hg experienced progressive stenosis and required intervention. There was no advantage in delaying intervention in the latter patient group.
Patients after surgical correction
Overall survival of patients after surgical correction of valvular PS is good, with survival rates of 90–96% 25 years after surgery (table 2).9–13 w7 If surgery is performed during childhood then survival is comparable to the normal population, while if repair of the stenosis is performed at adult age a 70% 25 year survival is described.8 Although survival is good, these patients do have residual lesions. Postoperative PR is common, especially if a transannular patch is used. Because PR is usually tolerated well for many years, reintervention is not often required in the first decades after surgery. In the long run, however, PR can lead to irreversible RV myocardial damage. Therefore, postoperative PR should be followed carefully. Indications for reintervention are summarised in figure 6.
: Post-interventional follow-up in patients with valvular pulmonary stenosis: an overview of published studies
Patients after balloon valvuloplasty
Long term outcome and survival after BPV are good, as is summarised in table 2.9 ,12–16 w8–w18 At mid-term follow-up (<2 years), restenosis, defined as an invasive gradient >50 mm Hg, is observed in 8–10% of patients. In the absence of severe annular hypoplasia and valvular dysplasia, this can be treated with a repeat BPV using a larger balloon with good success rates. Risk factors for restenosis are use of a relatively small balloon (balloon:annulus ratio <1.2) and an immediate invasive post-BPV gradient of ≥30 mm Hg. In the long term follow-up, the freedom of reintervention is reported as 88% and 84% at 5 and 10 years, respectively. Surgical intervention could be avoided in nearly all patients. PR was present in 40–90% of patients, with increasing prevalence over time. However, RV volume overload does not seem to be a major problem. The risk of significant PR seems to be related to younger age at treatment and smaller body surface area (BSA), more severe PS, use of a large or non-compliant balloon, and low residual gradient at the time of BPV.
Clinical follow-up
Patients with PS require lifelong follow-up with regular echocardiographic imaging, checking for the degree of PR, RV pressure, size and function and TR, unless their stenosis is mild (<36 mm Hg) and stable. Attention should also be paid to the occurrence of arrhythmias. Follow-up frequency depends on the severity of the lesion. Patients with mild PS, whether untreated or residual, require follow-up only once every 5 years. Patients with moderate PS or PR should be checked annually, including echocardiographic imaging every 2 years.
Endocarditis prophylaxis
Prophylactic use of antibiotics to prevent bacterial endocarditis is considered unnecessary, except in patients who have a valvular prosthesis, whether it is mechanical, autologous or biological.
Pregnancy and recurrence risk
Because the survival of patients with PS is good, many will reach reproductive age and will want to start a family. Questions about the haemodynamic burden of pregnancy, the impact on ventricular function, and the recurrence of PS in the offspring will thus be frequently encountered.
Recurrence risk
In isolated, non-syndromic PS the recurrence risk is reported to be 1.7–3.7%.17 w19 w20 In syndromic PS the recurrence risk will be higher, depending on the inheritance pattern of the specific syndrome. While the underlying genetic defect has been identified for the various syndromes associated with PS (table 1), this remains unknown for isolated valvular PS. Referral to the clinical genetics department should be offered to patients considering reproduction, especially when other family members also have a congenital defect.
Pregnancy in PS
In women with mild-to-moderate PS, either native or after previous correction, pregnancy is tolerated well. In severe PS, however, pregnancy may lead to right sided heart failure, due to the increased haemodynamic burden of pregnancy with an increase in cardiac output of 30–50%. Furthermore, atrial arrhythmias occur more frequently during pregnancy, especially in women with a previous history of such arrhythmias. These complications can occur regardless of the functional class before pregnancy. A decrease in ventricular function may occur and does not always resolve after pregnancy. In a Dutch retrospective study of 81 pregnancies in 51 women with mostly mild PS (New York Heart Association (NYHA) functional class I (almost 90% of patients) or II), cardiac complications occurred in 11 pregnancies (14%): two showed persisting deterioration of NYHA class (I>II), and in nine cases palpitations or arrhythmias were reported, but not investigated further. In a large review of the literature regarding cardiac and non-cardiac complications in pregnancy in women with congenital heart disease,18 there appeared to be no cardiac complications in women with PS, although the rate of hypertensive pregnancy complications was higher than in the general population.
Taking all this into account, there seem to be no grounds for discouragement of pregnancy in women with asymptomatic mild-to-moderate PS with a normal ventricular function, exercise tolerance and oxygen uptake. In women showing signs of reduced exercise tolerance or ventricular impairment, correction of the stenosis before conception should be considered. In severe PS, women should undergo correction before conception or they should be counselled against pregnancy. Women who are only discovered to have a significant PS during pregnancy should be followed in a tertiary centre. In the rare case of progressive right heart failure during pregnancy, BPV is the best treatment option. BPV can be performed with relatively low risk for the mother and child.19 Open heart surgery in pregnancy has a high risk of fetal complications or death, up to 30%.w21 w22
Pregnancy in PR
PR is often well tolerated in pregnancy. A London study of 76 pregnancies in 47 women with variable degrees of residual haemodynamic lesions of the RVOT showed that even in those with moderate-to-severe PR the pregnancy outcome was good. Predictors for right heart failure were twin pregnancy, branch PS, RV systolic dysfunction, and RV hypertrophy.20
Delivery
There will hardly ever be a cardiological indication for delivery by caesarean section. Unless women are in overt heart failure, vaginal delivery is safe.
Exercise and sports
Patients with mild PS and those without significant residual lesions after previous correction can live normal lives, without any exercise restriction. They should be allowed to participate in competitive sports. Patients with moderate PS and normal biventricular function can participate in moderate levels of exercise, and should be encouraged to do so. They should avoid competitive and static sports. In patients with severe PS, the stenosis must be resolved before they can resume unrestricted physical activity. While awaiting intervention they should be restricted to low intensity sports.
Patients with significant residual PR and RV dilatation should be considered for pulmonary valve replacement before increasing their level of physical activity. Timing of such an intervention depends on (systolic) ventricular function, volume and cardiac reserve, and their deterioration in time.
Conclusion
PS is a congenital heart defect with widely variable presentation. It usually can be treated well, with low risk. Nevertheless, patients can have or develop residual lesions and therefore most of them require lifelong cardiological follow-up.
Pulmonary stenosis: key points
-
The clinical picture of pulmonary stenosis (PS) varies widely, from critical stenosis in the newborn to lifelong asymptomatic mild stenosis.
-
The birth prevalence of PS seems to be increasing gradually and is highest in Asia.
-
PS can be part of an inheritable syndrome; if not, recurrence risk is 1.7–3.5%.
-
First choice treatment is balloon pulmonary valvuloplasty. It can be performed with low risk and has good long term results.
-
Patients with mild PS do not need exercise restrictions. Patients with more severe stenosis should avoid competitive and static sports.
-
Pregnancy in women with PS is generally well tolerated. The vast majority can go safely through pregnancy and delivery as long as adequate pre-pregnancy counselling and specialised high quality care during pregnancy and delivery are offered.
You can get CPD/CME credits for Education in Heart
-
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
-
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
-
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
-
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Acknowledgments
The authors wish to thank R Frowijn for his support in editing the illustrations.
References
- ↵An excellent review of all available evidence on the worldwide birth prevalence of congenital heart disease.
- ↵
- ↵Describes PR index as a very useful echocardiography tool for daily practice.
- ↵
- ↵
- ↵Nice overview of congenital cardiac surgery in a classic textbook.
- ↵These new developments in percutaneous valves might be promising but they first have to prove themselves.
- ↵Much cited classic reference on the long term outcome in PS patients.
- ↵
- ↵
- ↵
- ↵Very recent overview of the long term results of both BPV and surgery.
- ↵
- ↵Large multicentre registry on BPV in over 500 patients.
- ↵
- ↵
- ↵
- ↵A nice, recent overview on pregnancy outcomes in congenital heart disease patients. No cardiac events occurred in 100 pregnancies in PS patients.
- ↵
- ↵This study shows that the haemodynamic burden of PR is tolerated well in pregnancy, except when additional risk factors are present.
Footnotes
-
Contributors All authors have made significant contributions to the design, literature review and writing of this manuscript.
-
Competing interests In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article. The authors have no competing interests.
-
Provenance and peer review Commissioned; internally peer reviewed.