Article Text

Statistics from Altmetric.com
The rapid development of interventional procedures for the treatment of arrhythmias in humans, especially the use of catheter ablation techniques, has renewed interest in cardiac anatomy. Effective and safer catheter based procedures have come from an improved understanding of not only the gross anatomic details of the heart, but also some architectural and histological features of various cardiac regions and their neighbouring landmarks. This article aims to provide the basic anatomic information needed to understand mapping and ablative procedures for the cardiac interventional electrophysiologist.
Spatial locations of the cardiac chambers during an electrophysiological study
The correct attitudinal position and spatial relationships of the different cardiac structures should be understood. Viewed from the frontal aspect of the chest, the right ventricle (RV) is the most anteriorly situated cardiac chamber because it is located immediately behind the sternum. The cavity of the right atrium (RA) is anterior, while the left atrium (LA) is the most posteriorly situated chamber. Owing to the obliquity of the interatrial septum (IS) plane (which is at an angle of about 65° from the sagittal plane), and to the different levels of the mitral and tricuspid valve (TV) orifices, the LA is situated more posteriorly and superiorly than the RA.
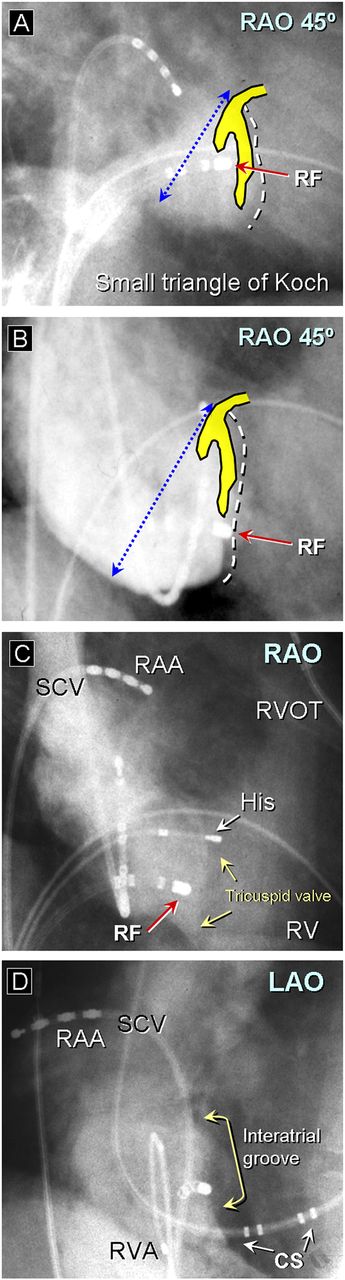
The introduction of non-fluoroscopic electroanatomic mapping technologies has enabled electrophysiologists to interpret correctly the gross morphology and attitudinal position of the cardiac chambers during the course of a mapping procedure.1 Intracardiac echocardiography has also been used to visualise some endocardial structures such as the oval fossa (OF) or terminal crest (TC) and to monitor the effects of ablation. In spite of these recent developments, conventional fluoroscopy remains the essential guide during an electrophysiological study and ablation procedure. Fluoroscopic examination is performed using the frontal and oblique projections. Two or more fluoroscopic views are usually needed to define the anatomic position in the heart and to estimate more accurately the location of the exploring electrode. The right anterior oblique (RAO) projection defines what is anterior, posterior, superior, and inferior. The left anterior oblique (LAO) defines the superior, inferior, anterior, and posterior locations for both the right and left atrioventricular (AV) grooves (figures 1 and 2). The LAO is also useful to define what is septal, permitting the differentiation between the complex right and left paraseptal regions. It is the preferred projection to catheterise the coronary sinus (CS) and its continuation along the epicardial aspect of the postero-inferior region2 (figures 1 and 2).

(A) Simulated (gross human specimens) and fluoroscopic right anterior oblique (RAO) projection showing electrode catheters placed at the right atrial appendage, bundle of His (His), right ventricular apex and coronary sinus (CS). (B) Simulated and fluoroscopic left anterior oblique (LAO) projection. The CS runs on the atrial side of the mitral annulus along the inferior wall of the left atrium towards the posterior border of the heart. Both RAO and LAO projections define what is anterior, posterior, superior and inferior. The LAO view serves to demonstrate in an attitudinal orientation the septal location permitting the differentiation between the right and left atrioventricular grooves. AO, aorta; CSo, coronary sinus ostium; ICV, inferior caval vein; LV, left ventricle; MCV; mid cardiac vein; P; pulmonary valve; RAA, right atrial appendage; RVA, right ventricular appendage; RVOT, right ventricular outflow tract; TV, tricuspid valve.

(A, B) Fluoroscopic 45° right anterior oblique projection showing the angiographic display of both the mitral valve and tricuspid valve (TV) during the injection of radiographic contrast into the right atrium (RA) and the left ventricle (LV). (C, D) Three dimensional spatial orientation of the cardiac chambers using the NavX system. (E) Opened RA and left atrium (LA) in a human specimen. Note the TV displaced apically in relation to the mitral valve (MV) and the apposition between the inferior/medial RA and the posterior region of the LV (double white arrow in panel E). The smooth circumferential area of atrial wall surrounding the orifice of the TV and MV is described as the vestibule. The trabeculated wall of the RA anterior to the terminal crest is the right atrial appendage (RAA) and contains multiple pectinate muscles (asterisk), which arise from the crest and extends all round the vestibule. CS, coronary sinus; ICV, inferior caval vein; LAA, left atrial appendage; LIPV, left inferior pulmonary vein; LSPV; left superior pulmonary vein; OF, oval fossa; PA, pulmonary artery; RV, right ventricle; RVOT, right ventricular outflow tract.
RA anatomy
The RA has four components: the venous component, the vestibule, an appendage, and it shares the septum with the LA.w1 The venous component is located posterolaterally and receives the systemic venous return from the superior caval vein (SCV), the inferior caval vein (ICV), and the coronary venous return from the CS. The vestibule is a smooth muscular wall around the tricuspid orifice, and supports the leaflets of the TV. The characteristic feature of the vestibule is that it is surrounded by the pectinate muscles of the RA. The right atrial appendage (RAA) lies over the anterosuperior aspect of the right AV groove and contains multiple pectinate muscles, which arise from the TC or crista terminalis (figures 2 and 3).

(A) Opened right atrium in simulated right anterior oblique view to show the most important landmarks and its four components. Note the oval fossa (OF) and the terminal crest which is a thick C-shaped muscular trabecula that distally ramifies to form the pectinate muscles. The Eustachian valve (asterisks) separates the inferior vena cava (IVC) from the inferior right atrial isthmus. The Thebesian valve (white arrow) guards the entry into the coronary sinus. (B) Four chamber section through the heart profiles showing the true interatrial septum (double red arrow); the remaining parts (dotted lines) mark the superior and inferior infolding of the atrial wall and the fibro-fatty sandwich of atrial and ventricular musculature posteriorly. (C) Short axis section across the atrial chamber below the flap valve of the OF. Note the atrioventricular valves, the vestibules (dotted lines), and the different shape and size of the atrial appendages. Ao, aorta; LAA, left atrial appendage; MV, mitral valve; RAA, right atrial appendage; RCA, right coronary artery; RVA, right ventricular apex; RVOT, right ventricular outflow tract; SCV, superior caval vein; TC, terminal crest; TV, tricuspid valve; VS, ventricular septum.
TC and the region of the sinus node
The TC is a significant structure in several forms of atrial tachyarrhythmias, acting as a natural barrier to conduction in common atrial flutter. The TC is a large muscular ridge that separates the smooth walled venous part (venous component) from the extensive trabeculated (pectinated) RAA. Thus, the C-shaped crest extends laterally and inferiorly, turning in beneath the orifice of the inferior vena cava (IVC) to ramify as a series of trabeculations in the area between the IVC and the TV3 (figure 3). The pectinate muscles, originating from the crest and extending along the wall of the appendage towards the vestibule of the TV, show a non-uniform trabecular pattern in most hearts. It is relevant the confluence between the TC at its origin in the interatrial groove and the origin of another important muscular fascicle, the interatrial Bachmann's bundle, which extends into the LA.3
The sinus node (SN) is the source of the cardiac impulse. It is usually localised within the TC at its anterolateral junction with the SCV. The SN is crescent-like in shape with an extensive longitudinal axis. Notably, it is not insulated by a sheath of fibrous tissue and varies in position and length along the crista terminalis. Sections through the SN also show a discrete area, composed of loosely packed myocytes, which we have termed the paranodal areaw2 (figure 4). While in 72% of the hearts the location of the nodal body is subepicardial, in the other 28% the inner aspect of the nodal body is more subendocardial.4 Its margin is irregular with multiple extensions interdigitating into the neighbouring working atrial myocardium (figure 4). Both inappropriate sinus tachycardia and sinus nodal re-entrant tachycardia are arrhythmias arising from the sino-atrial area. Box 1 shows the relevant anatomic determinants for SN ablation or modification with endocardial catheter techniques.
Right-sided atrial tachycardia and atypical right atrial flutter
Inappropriate sinus tachycardia: ablation along the crista terminalis
-
Broad location of the sinus nodal tissue
-
Potential cooling effect of the centrally located sinus nodal artery
-
Thickness of the terminal crest
-
Non-uniform pectinate trabeculations towards the TV
-
Risk of right phrenic nerve injury
Coronary sinus origin and near the AV node or His region
-
Endocardial and close anatomic proximity of the compact AV node
-
Variable position of the compact AV node within the right atrial AV junction
-
Cooling effect of the CS blood flow: proximity to the inferior AV nodal extensions
-
A better protected His bundle than the compact AV node against radiofrequency energy
Atrioventricular nodal reentrant tachycardia
-
Dimensions and spatial orientation of the triangle of Koch
-
Variable location of the His bundle recording site within the Koch's triangle
-
Variable position of the compact AV node and its inferior extensions
Isthmus dependent atrial flutter
-
Length of the cavo-tricuspid isthmus: shorter ‘central isthmus’
-
Endocardial geometry of the isthmus: deeper pouches (sub-Thebesian recess)
-
Obstacles such as a large Eustachian valve/ridge
-
Variable content of myocardial and fibro-fatty tissues at the ablation zone
-
Proximity of the AV nodal artery and right coronary artery
AV, atrioventricular; CS, coronary sinus; TV, tricuspid vestibule.

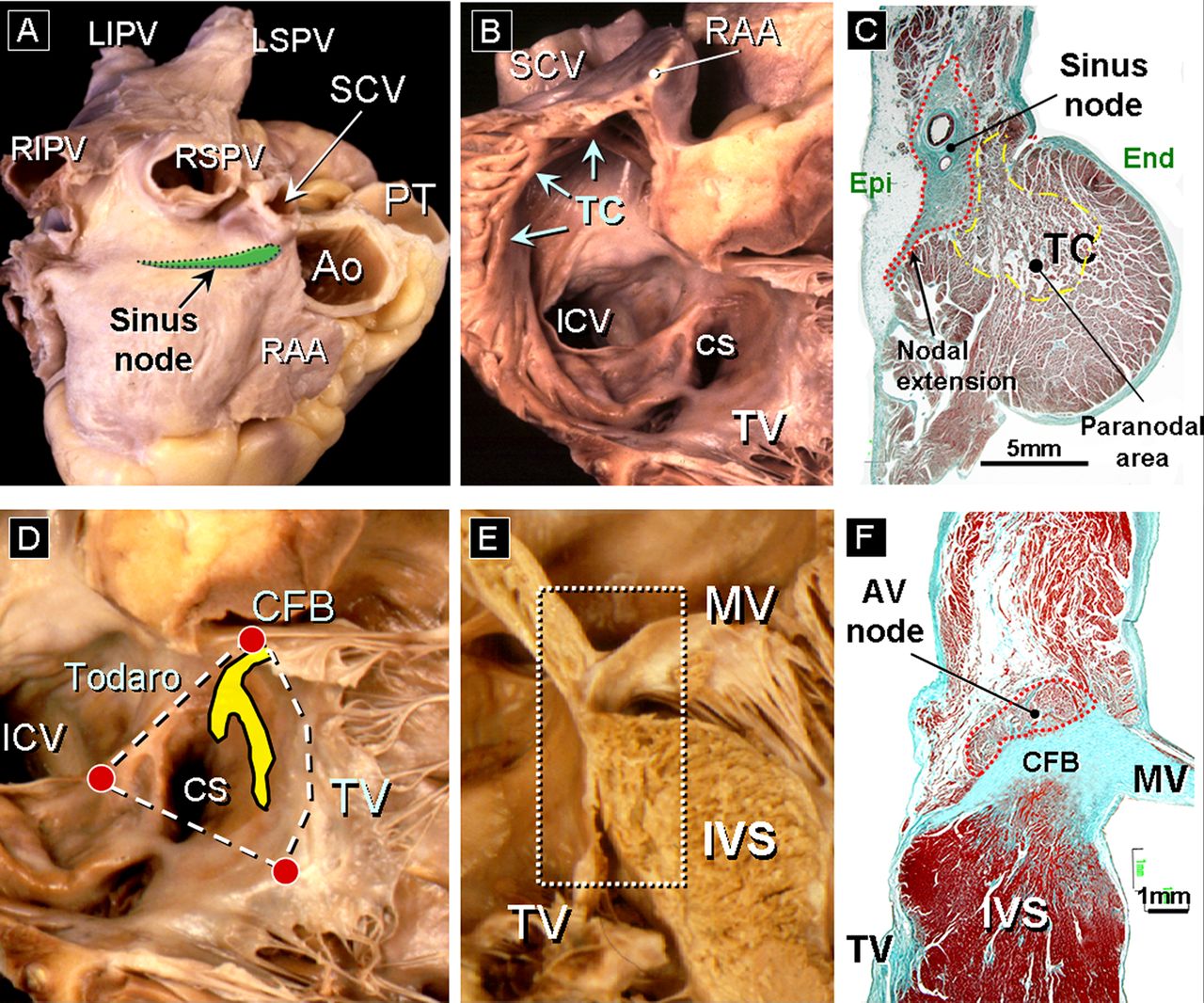
(A) Lateral view of the right atrium (RA) showing the location of the sinus node (SN) (fusiform green colour). (B) The RA is shown in right anterior oblique projection. The terminal crest arches anterior to the orifice of the superior caval vein, and the SN is located between themselves and extends toward the inferior caval vein. (C) Histological section of the SN body (Masson trichrome stain) within a dense matrix of connective tissue (green colour) and showing a nodal extension (arrow). (D) Endocardial view of the posterior and paraseptal walls of the RA showing the limits of the triangle of Koch. The apex of the triangle is the central fibrous body (CFB). The atrioventricular (AV) node is illustrated in yellow. (E) Four chamber section to show the different attachment of the mitral valve and tricuspid valve. (F) Histological section corresponding to the location of the AV node stained with Masson trichrome. Note the semi-oval shape of the compact AV node that lies over the CFB. Ao, aorta; CS, coronary sinus; Epi, epicardium; End, endocardium; ICV, inferior caval vein; IVS, interventricular septum; LIPV, left inferior pulmonary vein; LSPV, left superior pulmonary vein; MV, mitral valve; PT, pulmonary trunk; RAA, right atrial appendage; RIPV, right inferior pulmonary vein; RSPV, right superior pulmonary vein; SCV, superior caval vein; TC, terminal crest; TV, tricuspid valve.
Inferior right atrial isthmus and its anatomic determinant for atrial flutter ablation
The inferior right atrial cavo-tricuspid isthmus, a critical link for the macro-reentrant circuit of isthmus dependent atrial flutter, is the target of catheter ablation techniques that have become the treatment of choice for this arrhythmia. Anatomical and imaging studies have shown a wide range of morphologies and architectural factors at the isthmus level that may influence the feasibility of obtaining a complete, transmural and permanent ablation line across this anatomic landmark.5 w3 w4 (box 1). With the heart in an attitudinal orientation, we identified and measured the length of three levels of the isthmus: paraseptal (24±4 mm), inferior (19±4 mm), and inferolateral (30±3 mm).w3 The paraseptal isthmus forms the base of the triangle of Koch (figures 4⇓–6). The inferior isthmus is also known as the ‘central isthmus’ owing to its location between the other two isthmuses.6 The inferior isthmus represents the optimal target for linear ablation because this is the site where the orifice of the ICV is closer to the TV insertion, the wall thickness is minimal, and there is a larger distance to the right coronary artery and the AV node or its arterial supply6 (figure 6). Fluoroscopically, the 6 or 7 o'clock position in the LAO view correlates with the preferred site for ablation.
A, B) Right atrial angiograms in 45° right anterior oblique projection showing the tricuspid valve (TV) plane and the angiographic limits of the triangle of Koch. The position of the ablation catheter at the site of application of radiofrequency (RF) is shown. Note the variable dimensions of the triangle. The risk of atrioventricular (AV) nodal injury increases when the Koch's triangle is small. (C) Injection of contrast during the slow pathway ablation. Note the exact position of the ablation catheter close to the TV. (D) The left anterior oblique projection demonstrates that the ablation catheter (RF) has a septal location in relation to the interatrial groove. LAO, left anterior oblique; RAA, right atrial appendage; RAO, right anterior oblique; RV, right ventricle; RVOT, right ventricular outflow tract; SCV, superior caval vein.

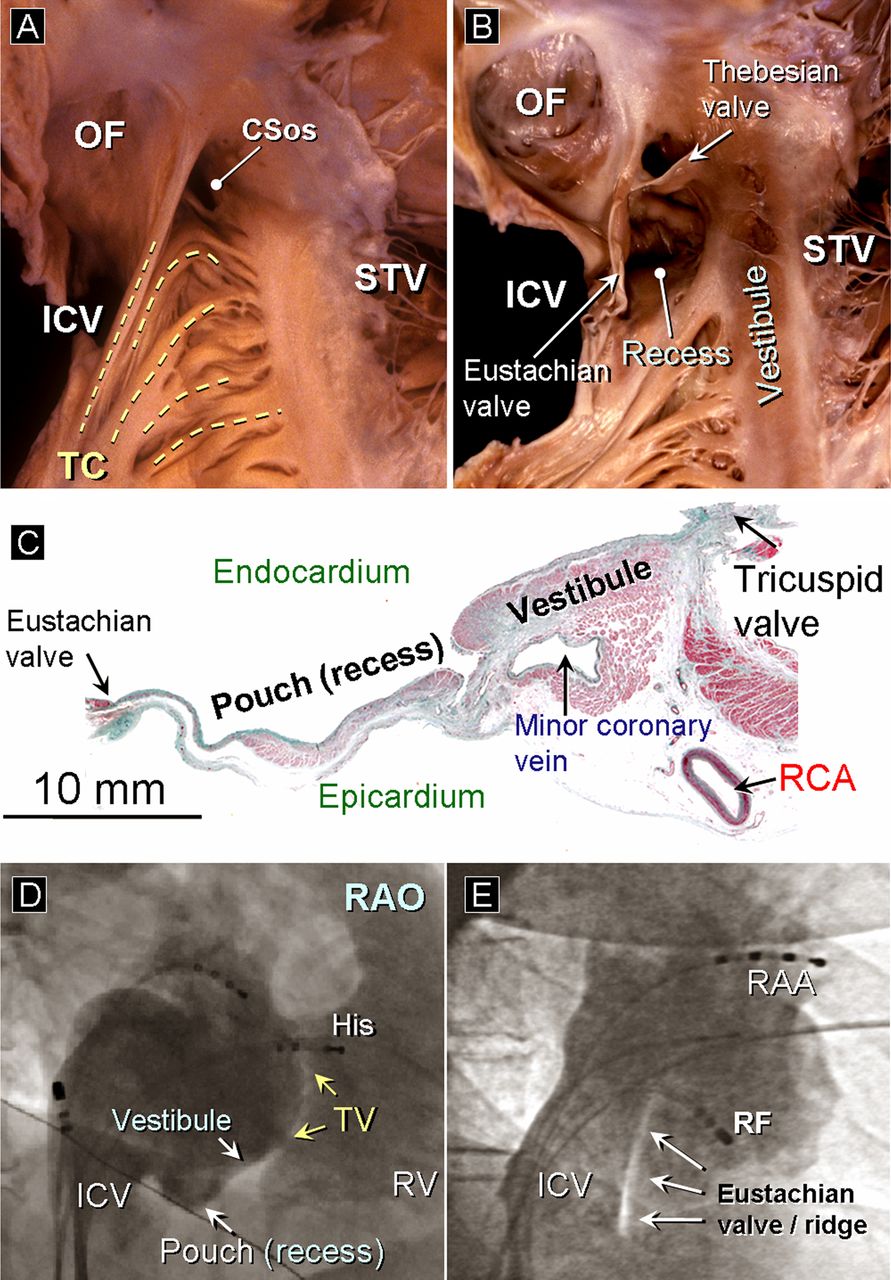
(A, B) The right inferior cavo-tricuspid isthmus is a quadrilateral area in the floor of the right atrium bounded by the inferior caval vein and the Eustachian valve posteriorly and by the septal attachment of the tricuspid valve (STV) anteriorly. Note in panel B the complex endocardial topography of the isthmus with thicker trabeculations from the terminal crest and a deep sub-Thebesian recess (pouch). (C) Sagittal histological section with Masson trichrome at the level of the central isthmus. Note the proximity of the minor coronary vein and the right coronary artery to the endocardium of the vestibule. The section shows the variable content of myocardial and fibro-fatty tissues with a thicker anterior vestibular area. (D, E) Right atrial angiograms in the right anterior oblique projections that show in panel D a large and deep pouch recess and in panel E a thicker Eustachian valve and ridge, anatomic obstacles that may complicate isthmus ablation (radiofrequency). CSos, coronary sinus ostium; ICV, inferior caval vein; OF, oval fossa; RAA, right atrial appendage; RAO, right anterior oblique; RCA, right coronary artery; RF, ablation catheter; RV, right ventricle; TV, tricuspid valve.
Architectural insights of the triangle of Koch for catheter ablation
The triangle of Koch contains the AV node and its inferior extensions.7 It is bordered posteriorly by a fibrous extension from the Eustachian valve and by a ridge called the tendon of Todaro. The anterior border is demarcated by the attachment of the septal leaflet of the TV (figure 4). The apex of this triangle corresponds to the central fibrous body (CFB) where the His bundle penetrates. The base of the triangle is the orifice of the CS, and the vestibule of the RA immediately anterior to it. The area of the triangle is targeted for ablation of the slow nodal pathway. In addition, it is commonly the seat of the atrial insertions of septal and paraseptal AV accessory pathways and certain forms of atrial tachycardia. The dimensions and spatial orientation of this right atrial region vary considerably, which is clinically relevant in the case of catheter ablation procedures largely guided by anatomic landmarksw5 (figure 5). Energy current applied near the compact AV node must be avoided. The induction of AV block during ablation of the slow pathway is more likely to occur when the triangle is small, not only because there is less space to apply energy current safely without impinging upon the area immediately overlying the inferior extensions or compact node, but also because there is little margin for error with regard to stability of the tip of the catheterw6 (box 1).
The AV node consists of a compact portion and an area of transitional cells. The compact portion lies over the CFB at the apex of the triangle (figure 4). The compact AV node contains rightward and leftward inferior extensions, with the right extension close to the tricuspid annulus.8 w7 The AV node continues distally with the His bundle. During an electrophysiological study the site of the largest His bundle electrogram recording does not always coincide with the antero-superior vertex of the triangle.7 Therefore the position of the compact AV node and its inferior extensions just proximal to the His bundle vary within the landmarks of the triangle. The penetrating His bundle can readily be distinguished from the compact node at the point where the conduction axis itself becomes completely surrounded by tissues of the CFB.7 Thus the bundle of His is better protected than the compact node against radiofrequency energy.
Paraseptal region and inferior pyramidal space
The previously called posteroseptal region is in fact inferior and paraseptal, because it is inferior to the true atrial septum. Therefore the term ‘infero-paraseptal’ would be more anatomically correct. The complex inferior paraseptal region represents the confluence of all four chambers (the so-called inferior pyramidal space) and the CS.7 The pyramidal space is an area whose superior vertex is the CFB, the lateral sides are formed by the convergence of the left and right atria, and whose floor is the muscular ventricular septum (VS) and left ventricle (LV). The CS limits the base of this area, which has a pyramidal configuration. Tissues that are continuous with the inferior epicardial AV groove occupy the pyramidal space together with the AV nodal artery and the proximal CS with the middle cardiac vein and posterior coronary vein (figure 7).
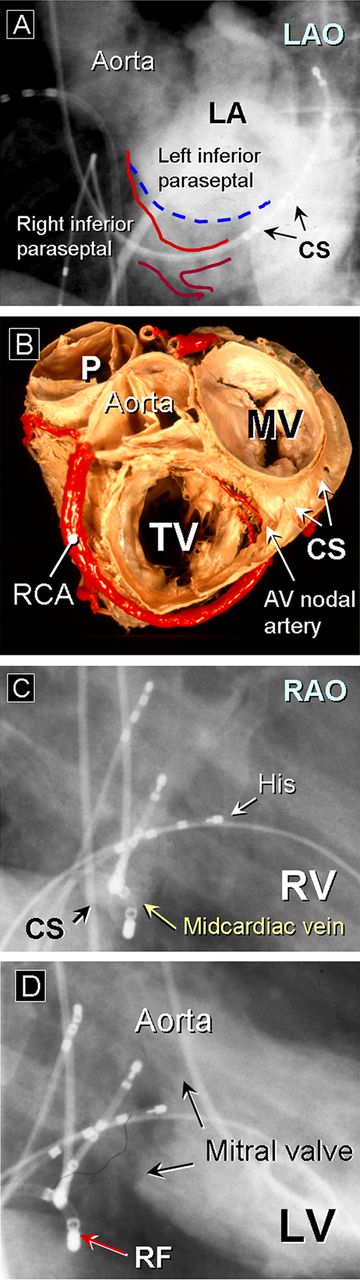
(A) Left atrial angiography throughout a transseptal puncture in the left anterior oblique projection (LAO). The LAO projection makes it possible to define the anatomic relation between the right and left paraseptal regions and the fluoroscopic limits of the inferior pyramidal space. Note the variable relation of the coronary sinus (CS) catheter and the atrial side of the mitral annulus. (B) Heart specimen in simulated LAO projections showing the right and left atrioventricular (AV) groove. The convergence of the left and right atria forms the lateral side of the inferior pyramidal space; the superior vertex is the central fibrous body and the CS limits the base of this space. Note the AV nodal artery originates from the apex of the U-turn of the distal right coronary artery and penetrates into the base of the inferior paraseptal region (inferior pyramidal space) at the level of the crux of the heart. (C, D) Right anterior oblique (RAO) projection. Ablation of an inferior paraseptal accessory pathway within the mid cardiac vein (MCV) using the CS myocardial sleeve as connection between the atria and ventricle. The MCV end ups in the proximal CS and runs an inferior course before bending anteriorly along the epicardial surface of the muscular interventricular septum. LV, left ventricle; MV, mitral valve; P, pulmonary trunk; RCA, right coronary artery; RF, ablation catheter; RV, right ventricle; TV, tricuspid valve.
The mid septal region corresponds to the floor of Koch's triangle between the His recording location and the anterior portion of the CS ostium. In this region, because the TV is displaced apically and inferiorly in relation to the mitral annulus, there is an apposition between the inferomedial RA and the posterior region of the LV (figure 7). In addition there is no atrial septum in the region of the His bundle at the apex of Koch's triangle (formerly anteroseptal). Thus this area is more properly regarded as being supero-paraseptal (box 2).
Accessory atrioventricular connections
Left free-wall accessory pathways
-
Fibrous tissue around the MA interposed between the atrial and ventricular myocardium
-
Basal cords of ventricular myocardium on the ventricular side of MA
-
Aortic–mitral valve continuity (anterior limit of the left free wall)
-
The CS as guidance for MA: variable separation of the CS from the annulus
Right free-wall accessory pathways
-
The TA is displaced apically in relation to the MA
-
Less developed fibrous tissue and frequently discontinuous TA
-
Acute angulation of the tricuspid leaflets towards the ventricle
Inferior paraseptal accessory pathways (‘posteroseptal’)
-
Complex relation between the right and left inferior paraseptal region
-
Musculature over the coronary venous system: coronary sinus diverticulum
-
The AV nodal artery towards the compact AV node along the inferior paraseptal area
-
The inferior extension of the compact AV node
Supero-paraseptal accessory pathways (‘anteroseptal’)
-
Proximity to normal conduction system
-
Variable extension of the central fibrous body: the region of the His penetrating bundle
-
Discontinuous fibrous tissue around the tricuspid annulus (superior limit)
Mid septal accessory pathways
-
Area between the His recording location and the anterior portion of the CS ostium
-
Apposition between the inferior/medial RA and posterior region of the left ventricle
-
Similar anatomic determinants to the slow pathway ablation
CS, coronary sinus; MA, mitral annulus; RA, right atrium; TA, tricuspid annulus.
INTERATRIAL SEPTUM and interatrial muscular connections
The true IS is the OF, a depression in the right atrial aspect of the area traditionally considered to be the IS. The antero-inferior buttress, which anchors the flap valve of the OF into the AV junctions, is also a septal structure. The buttress is confluent with the floor of the triangle of Koch, but as mentioned above this is not a septal area. The buttress, in contrast, forms a direct muscular boundary between the atrial cavities. The remaining parts of the ‘septal’ aspect are formed by the infolded right atrial wall superiorly and inferiorly, and the fibro-fatty sandwich of atrial and ventricular musculature anteriorly9 (figure 8). The muscular fold forming the rim of the oval foramen itself is filled with fibro-fatty tissues of the epicardium and termed the interatrial groove (or septal raphe). Superiorly and posteriorly, this is the posterior interatrial groove. On the left atrial side, the valve is usually indistinguishable from the parietal atrial wall apart from a small crescent-like edge that marks the site of its free margin, the last part of the valve to become adherent to the rim. Transseptal punctures to access the LA should be performed through the OF. Also relevant is the spatial relationship between the anterior atrial wall or the plane of the atrial septum and the root of the aorta (figure 8). An accidental puncture throughout the interatrial groove may result in haemopericardium in highly anticoagulated patients.

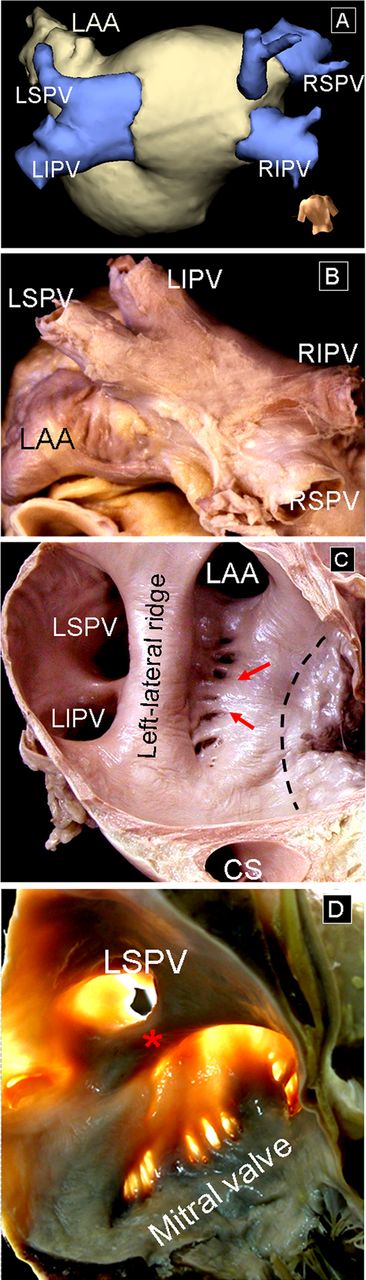
(A) Dissection of the posterior wall of the left atrium (LA) close to the posterior interatrial groove. The smooth walled venous component of the LA is the most extensive. The septal aspect of the LA shows the crescentic line of the free edge of the flap valve (green dotted line) against the rim of the oval fossa (OF). The orifices of the right superior and inferior pulmonary veins (RSPV and RIPV) are adjacent to the plane of the septal aspect of the LA. (B) Longitudinal sections showing the orifices of the right pulmonary veins. Note the relation of the superior vena cava to the RSPV and right pulmonary artery. (C) The dome or roof of the LA has been removed and the left atrial side of the septum can be seen by transillumination of the OF. In the case of patent foramen oval, the LA can be accessed from the right atrium (RA) through a crevice (blue dotted line) that is the last part of the valve to be sealed to the rim. (D) Short axis through the interatrial septum (green arrow). Note by transillumination the so-called left atrial ridge that is a fold in the LA wall between the left atrial appendage and the left pulmonary veins. (E) Histological section with Masson trichrome taken through the short axis of the heart to show the thin flap valve and the muscular rim of the fossa. Note the non-uniform thickness of the left atrial wall and the close relationship of the anterior wall of the RA with the transverse sinus and aorta (Ao). ER, Eustachian ridge; LAA, left atrial appendage; LIPV, left inferior pulmonary vein; LSPV, left superior pulmonary vein; MV, mitral valve; PT, pulmonary trunk, RAA, right atrial appendage; RI, right inferior pulmonary vein; RPA, right pulmonary artery; RS, right superior pulmonary vein; SCV, superior caval vein; TV, tricuspid valve.
Apart from a muscular continuity at the rim and floor of the OF, there are multiple muscular bridges between the atrial chambers.9 The anterior right atrial wall is mainly formed by chains of cardiomyocytes aligned with their long axes in similar orientation that run parallel to the AV groove (figure 9). A prominent band of these cardiomyocytes is the Bachmann's bundle that can be traced from the superior cavo-atrial junction leftward to become the superficial fibres of the LA, crossing the anterior interatrial groove. This band is the most prominent muscular interatrial bridge.9 w8 Additionally, in some hearts the Bachmann's bundle may coexist with muscular bridges across the posteroinferior interatrial groove. Also connections between the muscular wall of the CS and the LA are common.9

(A–C) In these specimens the epicardium has been removed to show the arrangement of the myocardial strands in the superficial parts of the walls. In panel A an interatrial muscle bundle or Bachmann bundle is present in this heart. Panel B is a view of the roof and posterior wall of the left atrium (LA) showing the myocardial strands (septopulmonary bundle) in the region between the left and right pulmonary veins (PVs). Panel C is a view of the posterior wall of the LA with transillumination to demonstrate the non-uniform myocardial thickness of the LA wall. (D) Cross histological section stained with elastic van Gieson of the LA, PVs and the superior vena cava. Also note the variable myocardial content of the walls of the LA and the epicardial location of vegetative nerves and ganglia. (E) Cross histological section of the left PVs stained with Masson trichrome. Note the inter-PV myocardial connections (arrow) between the superior and inferior veins. Ao, aorta; Epi, epicardium; ICV, inferior caval vein; LAA, left atrial appendage; LIPV, left inferior pulmonary vein; LPA, left pulmonary artery; LSPV, left superior pulmonary vein; LV, left ventricle; RAA, right atrial appendage; RIPV, right inferior pulmonary vein; RSPV, right superior pulmonary vein; SCV, superior caval vein.
Left atrial anatomy relevant to catheter ablation
Ablation techniques in patients with atrial fibrillation (AF) have evolved from rather limited initial approaches to quite extensive left atrial intervention (box 3). From a gross anatomical viewpoint the LA possesses a venous component that receives the pulmonary veins (PVs), a vestibule, an appendage, and the so-called IS (figure 8). In reality, both atriums also possess a body. This is best seen in the LA, and is the smooth walled component between the vestibule and the venous component. The body of the RA is much smaller, and represents the space between the left venous valve, when this structure can be recognised, and the atrial septum. The major part of the LA, including the septal component, is smooth walled except for the ostium of the atrial appendage and its neighbouring structures.10 The walls of the LA can be described as superior, posterior, left lateral, septal (or medial), and anterior. The anterior wall that is immediately inferior to the Bachmann's bundle, located just behind the aorta, can be very thin and measures approximately 1–2 mm in thickness transmurally. The superior wall, or dome, is thicker compared with the posterior and postero-inferior walls, measuring 3.5–6.5 mm.11 ,12
Atrial fibrillation and left atrial flutter. Ventricular tachycardias
Dimensions and non-uniform myocardial thickness of the LA
-
Variant anatomy of the PVs: length of the common pulmonary trunk
-
Inter-PVs myocardial connections (some epicardially located)
-
Endocardial ridges: the left atrial ridge and the interpulmonary isthmus (PV carina)
-
Extra-appendicular pectinate muscles (mitral isthmus and vestibule)
-
Cooling effect by the intramyocardial atrial arteries
-
Autonomic nervous system on the epicardial surface of the LA wall
-
Fibrous tissue around the mitral annulus
-
Proximity with phrenic nerves, oesophagus, vagus nerve and left circumflex artery
-
The true atrial septum: transseptal punctures to access the LA
-
Spatial orientation of the interatrial groove and plane of the atrial septum
-
Thickness of the flap valve: fibrous/muscular rim (septum primun)
-
Patent foramen oval/aneurysmal oval fossa
-
Relation with the aortic root and transverse pericardial sinus
-
Ventricular outflow tract tachycardias
-
Myocardial extension above the anatomic ventriculo-arterial junctions
-
Proximity of the AV conduction: aortic–mitral valve continuity (LVOT)
-
Extension of the supraventricular crest (RVOT)
-
Variable septo-marginal and septo-parietal trabeculations (RVOT)
Epicardial ablation
-
Overlying epicardial fat: varying presence of epicardial adipose tissue
-
Proximity to epicardial coronary vessels, pericardiophrenic vessels and phrenic nerve
-
Local variation of pericardial reflections
AV, atrioventricular; LA, left atrium; LVOT, left ventricular outflow tract; PV, pulmonary vein; RVOT, right ventricular outflow tract.
PVs and their venoatrial junctions
The LA posterior wall is the anatomical location of the venous component and contains the venoatrial junctions of the PVs, with the left veins located more superiorly than the right veins (figures 9 and 10). The superior PVs run cranially and more anteriorly, whereas the inferior veins have a more posterior and lateral course. Usually the right superior PV passes behind the junction between the RA and the superior vena cava (SVC) whereas the inferior PVs pass behind the intercaval area.12 The orifices of the right PVs are directly adjacent to the plane of the atrial septum. The most common anatomic variants (30–35%) of the PVs ending in the LA include a conjoined homolateral ostia of the left PVs (25% of specimens) and a supernumerary or additional right PV (figure 10). It is important to note that: (1) the PV ostia are not round but ovoid; (2) the PV size varies over the cardiac cycle and respiration; and (3) the transition from the atrial endocardium to the venous endothelial layer is smooth with an unclear anatomic border. Thus, identification of the PV ostia may be difficult in some patients.

(A) Three dimensional reconstruction of the left atrium (LA) and pulmonary veins using the NavX system from data obtained with a 32 slice multidetector CT scanner to show conjoined ostia, a common variant seen in up to 25% of cases, on the left side, and a separate right middle pulmonary vein (PV), which drains the middle lobe of the lung. (B) Human necropsy specimen showing the superior and posterior walls of the LA were anchored by the entrance of one PV at each of the four corners. (C, D) Endocardial left atrial wall in two postmortem heart specimens showing prominent left lateral ridges, extending in panel C (transillumination) to the inferior margin of the left inferior pulmonary vein and in panel D (asterisk) to the inferior margin of the left superior pulmonary vein. Note in panels C and D the extra-appendicular posterior pectinate muscles extending inferiorly from the left appendage toward the vestibule of the mitral valve (red arrows), and note the thinnest muscular wall in between the muscular trabeculae. CS, coronary sinus; LAA, left atrial appendage; LIPV, left inferior pulmonary vein; LSPV, left superior pulmonary vein; RIPV, right inferior pulmonary vein; RSPV, right superior pulmonary vein.
Atrial sleeves of non-uniform thickness, which are made up of working atrial myocardium, extend over the veno-atrial junction into the PV walls, and are more pronounced in the superior PVs.13 Specialised cells, particularly node-like cells, were not seen in our studies.11–13 Bridges of atrial myocardium and crossing strands have been observed connecting the superior and inferior PV, occurring more frequently between the left veins than between the right veins.12 w9
Lateral ridge and left atrial appendage
The left lateral ridge between the orifices of the left PVs and the mouth of the left atrial appendage (LAA) is the most relevant structural prominence on the LA endocardium.14 This structure is actually an infolding of the lateral atrial wall protruding into the endocardial LA surface as a prominent crest or ridge (figure 10). The ridge extends along the lateral wall of the LA from the anterosuperior to the postero-inferior region. Epicardially, this broad bundle is in continuity with the uppermost and distal part of the interatrial band (Bachmann's bundle). Within the fold runs the remnant of the vein of Marshall, together with abundant autonomic nerve bundles and a small atrial artery, which in some cases is the sinus nodal artery.14
The LAA tends to have a tubular shape with one or several bends resembling a little finger.w10 On the endocardial aspect, the orifice of the LAA is not perfectly round. Instead, it is oval in shape with a mean long diameter of 17.4±4 mm and a short diameter of 10.9±4.2 mm.12 A complicated network of fine pectinate muscles lines the endocardial aspect.w11 In between the muscle bundles the wall is paper thin. In some specimens (28%), muscular trabeculations can be found extending inferiorly from the appendage to the vestibule of the mitral valve (MV) (figure 10). These extra-appendicular myocardial bands correspond to the small posterior set of pectinate muscles originating from the myocardial bundles to embrace the LAA.14 In those hearts with extra-appendicular posterior pectinate muscles, the area in between the muscular trabeculae and the atrial wall becomes exceptionally thin (0.5±0.2 mm), increasing the risk of cardiac perforation during ablation in this zone.14 The isthmus of muscle between the orifice of the inferior PV and the mitral annulus is commonly dubbed the left atrial isthmus or mitral isthmus.w12 In this region, the vestibule directly apposes the wall of the great cardiac vein and its continuation, the CS10 ,12 (figure 10). In cases where the wall at the transition of vein to sinus is particularly muscular, it adds to the thickness of the isthmus. Frequently, the venous/sinus musculature is continuous with the left atrial wall. The mitral isthmus may also contain extra-appendicular posterior pectinate muscles.
Coronary sinus
The CS, which is the continuation of the great cardiac vein, runs on the atrial side of the true annulus along the postero-inferior wall of the LA.10 ,11 This separation from the annulus is more pronounced in the proximal 20 mm of the CS.w13 In all specimens, the venous wall of the CS is surrounded by a cuff of myocardium extending 40±8 mm from the ostium.w14 Myocardial connections varying in number and morphology leave this coronary muscle cuff and connect to the LA. The ostium of the CS abuts the superior margin of the right atrial-left ventricular sulcus and the inferior paraseptal mitral annulus in the pyramidal space (figures 7, 9 and 11). The inferior interatrial connections through the CS may explain the need for additional ablation in and on the CS to complete left atrial ablation lines extending down to the mitral annulus in this area for curing AF.w14

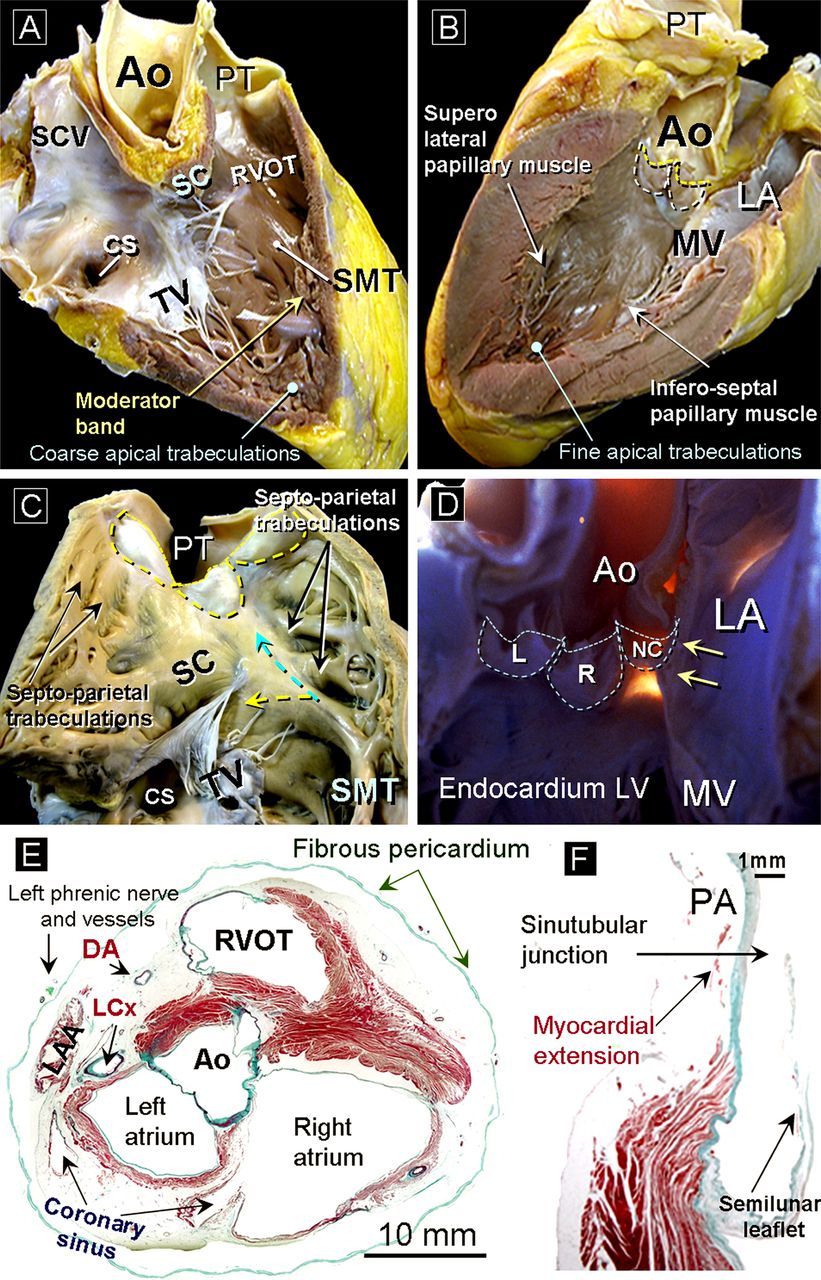
(A) Window dissection of a heart prepared by removing the anterior superior wall of the right ventricle (RV). The three components of the RV are revealed: the inlet (tricuspid valve (TV)), apical trabecular, and right ventricular outflow tract (RVOT) or infundibulum. Note the location of the supraventricular crest and septomarginal trabeculation (SMT). The body of the SMT continues as an important muscular strand, the moderator band, to the anterior papillary muscle and the parietal wall of the RV. (B) Sagittal section through the parietal wall of the left ventricle that shows the subaortic outflow tract and how the papillary muscles of the mitral valve closely face each other. (C) The anterior wall of the RV is opened to show the leaflets of the pulmonary trunk mainly supported by the RVOT; however, at the level of their commissures the leaflets are attached to the pulmonary artery trunk. The SMT (septal band) consists of a body and two limbs anterior and posterior. The anterior limb extends along the infundibulum (blue dotted arrow) and the posterior limb runs toward the TV (yellow dotted arrow). The septo-parietal trabeculations take their origin from the anterior margin of the SMT and extend along the parietal ventricular wall of the infundibulum. (D) Left ventricular endocardial view to show the membranous septum by transillumination. This is the point of emergence of the left bundle of His. The yellow arrows show the mitro-aortic continuity. (E) Cross histological section stained with Masson trichrome through the left and the right atria. Note the anatomic relation of the RVOT with the subaortic outflow. Also note the close proximity to the epicardial coronary vessel, the left phrenic nerve and the left atrial appendage, relevant during the epicardial approach for arrhythmia ablation. (F) Histological section of the pulmonary valve stained with Masson trichrome shows the attachment of the pulmonary leaflet. Note the myocardial extension above the sinotubular junction. Ao, aorta; CS, coronary sinus; DA, descending artery; L, left coronary sinus; LA, left atrium; LCx, left circumflex artery; LV, left ventricle; MV, mitral valve; NC, non-coronary sinus; PA, pulmonary artery; PT, pulmonary trunk; R, right coronary sinus; SC, supraventricular crest; SCV, superior caval vein.
The CS musculature may form extensions over the proximal portion of the middle cardiac vein and posterior cardiac vein. The oblique vein of Marshall (diameter 0.4–1.8 mm), located between the LAA and the left upper and lower PVs, runs inferiorly along the postero-inferior atrial wall to join the CS. In most hearts (70%), the oblique vein is <3 mm from the endocardium of the LA and has muscular connections to the left PVs.14
Right and left ventricles
In contrast to the conical morphology of the LV, the RV is more triangular in shape when viewed from the front and it curves over the LV.15 The geometry of the RV is also influenced by the convexity of the VS toward the RV in both systole and diastole under normal loading conditions. Both the RV and the LV have been described as having three components: the inlet (inflow tract), apical trabecular, and outlet portions (outflow tract) (figure 11). Morphologically, the RV is distinguished from the LV by having coarser trabeculae, a moderator band, and a lack of fibrous continuity between its inlet and outflow valves. The muscular trabeculations in the apical part of the RV are coarser than those in the LV.15 ,16 The apical trabeculations of the LV are fine and display a criss-cross pattern. The inlets also differ notably in the normal ventricles, as do the outlets. Thus, the TV, possessing inferior, septal and antero-superior leaflets, has extensive chordal attachments to the VS, and is supported by notably eccentric papillary muscles. The MV possesses two leaflets, located anteriorly and posteriorly but positioned obliquely within the LV, and closing along a solitary zone of apposition. The anterior leaflet of the MV is separated from the septum by the subaortic vestibule, having fibrous continuity with two of the leaflets of the aortic valve.
Anatomy of the outflow tracts: implication for ablation of ventricular tachycardias
Premature ventricular contractions, ventricular tachycardias (VTs) and initiating beats for ventricular fibrillation have all been localised at the level of the right and left ventricular outflow tracts (RVOT and LVOT).w15 w16 Absence of structural heart disease is the rule with these arrhythmias.17
The majority of RVOT tachycardias originate in the superior, septal and anterior aspects of the infundibulum just underneath the pulmonary valve (box 3). The RVOT (outlet portion of the RV or the infundibulum) is a muscular structure of variable length (range 13–24 mm) that supports the semilunar leaflets of the pulmonary valve.15 Its posterior and inferior part consists of a prominent muscular crest, called the supraventricular crest (SC), that separates the inflow and outflow components of the RV (figure 11). The SC is in contact with the posterior part of the LVOT, as it inserts into the interventricular septum. On the septal aspect, this crest inserts between the limbs of the septomarginal trabeculation (SMT), or septal band.15 This muscular strap reinforces the septal surface of the RV, breaking up at the apex to form the moderator band and the anterior papillary muscle. The moderator band incorporates the right bundle branch, as conduction tissue fibres move towards the apex of the ventricle before entering the anterior papillary muscle.16 The septo-parietal trabeculations take their origin from the anterior margin of the SMT and run round the parietal ventricular wall of the infundibulum.15 These trabeculations show a variable extension (between five and 22 trabeculations) and thickness (range 2–10 mm) along the right and left septo-parietal wall of the RVOT.
All these structures are absent from the LV, where the outlet (LVOT) is much more reduced in size because of the fibrous continuity between two of the leaflets of the aortic valve and the aortic leaflet of the MV. Therefore, in the LV there is no muscular separation between inflow and outflow tracts.16
Although the two ventricular outlets have important differences in their structure, they also have one feature in common, namely the semilunar attachment of their leaflets. Because of the semilunar shape of the pulmonary leaflets this valve does not have a ring-like annulus.15 ,16 The semilunar hinges of the arterial valve leaflets extend proximally beyond the anatomic ventriculo-arterial junction, such that crescents of myocardium are incorporated into the bases of all three valvar sinuses of the pulmonary valve, and into two of the three aortic sinuses of Valsalva (figure 11). We observed in histological sections the existence of myocardial extensions or myocardial remnants on the epicardial aspect above the sinotubular junction in 20% of human specimens, showing continuity with the myocardium of the RVOT (figure 11). These extensions could justify the existence of idiopathic supravalvular tachycardia.
Pericardial space and neighbouring structures of the heart
The heart and its adjoining great vessels are enclosed in a sac, the parietal (fibrous) pericardium.w17 Superiorly, the fibrous pericardium is continuous with the adventitia of the great vessels. Within the fibrous pericardium there is a delicate double layered membrane known as the serous pericardium. One layer of the serous pericardium is fused to the fibrous pericardium while the other layer lines the outer surface of the heart and continues over the surfaces of the vessels as the visceral pericardium. Over the great vessels, the junctions between the two layers are the pericardial reflections. The pericardial cavity is the space between the layers of the serous pericardium.
There is a small area behind the lower left half of the body of the sternum and the sternal ends of the left fourth and fifth costal cartilages where the fibrous pericardium is in direct contact with the thoracic wall. This area allows the pericardial space to be accessed.w18 The pericardial cavity has two main sinuses and several recesses.18 These are not complete compartments but represent extensions of the cavity. The transverse sinus is delineated anteriorly by the posterior surface of the ascending aorta and pulmonary trunk bifurcation and posteriorly by the anterior surface of the atria (figure 12). The oblique sinus, a large cul-de-sac behind the LA, is formed by the continuity between the reflections along the PVs and caval veins.18 The right and left pulmonary venous recesses are at the back of the LA between the superior and inferior PVs on each side, indenting the side walls of the oblique sinus to a greater or lesser extent. The pericardial reflections at the veins, particularly the PVs, are varied and they can restrict access around the veins.18 The inferior and superior aortic recesses are extensions from the transverse sinus. The superior recess lies between the ascending aorta and the RA, whereas the inferior recess between the aorta and the LA extends to the level of the aortic valve.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Schematic drawing showing the superior, transverse and oblique sinuses. The fibrous pericardium is coloured in orange and the parietal layer of the serous pericardium in blue. The white area represents the reflections where the serous pericardium is continuous with the fibrous pericardium. (B) This dissection of a cadaver viewed from the front shows the transverse and oblique sinuses following removal of the heart. (C–E) Cross sections in three different specimens to show the close anatomic relationship of the oesophagus with the posterior left atrial wall (D) and the right and left veno-atrial junction (D and E). (F) The course of the right phrenic nerve is closely related to the superior cavo-atrial junction and the orifice of the right superior pulmonary vein. (G) The left phrenic nerve in its course has a close anatomic relationship with the left atrial appendage and the lateral wall of the left ventricle to penetrate into the left part of the diaphragm close to the apex of the ventricle. Ao, aorta; Es, oesophagus; ICV, inferior caval vein; LA, left atrium; LAA, left atrial appendage; LIPV, left inferior pulmonary vein; LSPV, left superior pulmonary vein; LV, left ventricle; PT, pulmonary trunk; RB, right bronchus; RIPV, right inferior pulmonary vein; RPA, right pulmonary artery; RSPV, right superior pulmonary vein; SCV, superior caval vein.
The close anatomic vicinity of the cardiac chambers to important structures and the regional distribution of the autonomic nervous system elements that may be affected by interventional manoeuvres should also be understood by the electrophysiologist (figures 11 and 12). Preganglionic parasympathetic and postganglionic sympathetic fibres come together into the fat pads of fatty tissues, and ganglionated plexuses populate the subepicardium. Abundant nerves and ganglions of the autonomic nervous system are present at the junction between the PVs and the LA with differential patterns of innervation.w19 w20
The oesophagus descends in virtual contact with the posterior wall of the LA (figure 12). Behind the posterior left atrial wall is a layer of fibrous pericardium and fibro-fatty tissue of irregular thickness that contains oesophageal arteries and the vagus nerve plexus.19 Understanding the course of the oesophagus is essential to reduce the risk of atrio-oesophageal fistula during the left atrial ablation procedure. Thermal injury during endocardial LA may also involve the peri-oesophageal nerves,w21 resulting in an acute pyloric spasm and gastric hypomotility as an extracardiac adverse effect of AF ablation.
The right phrenic nerve has a close anatomic relationship with the SVC and the right PVs20 (figure 12). Consequently, catheter ablation techniques aimed at modifying the SN function at the lateral RA, and AF ablation at the orifice and adjacent area of the right superior PV, carry a certain risk of injuring the right phrenic nerve.20 Our study on cadavers also revealed that the course of the left phrenic nerve and its accompanying pericardiophrenic vessels in the fibrous pericardium were overlying the atrial appendage in the majority of cases20 w22 (figures 11 and 12).
You can get CPD/CME credits for Education in Heart
-
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
-
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
-
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
-
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Acknowledgments
The authors thank Drs Gonzalo Pizarro and Margarita Murillo for their contribution to the preparation of this article.
References
- ↵
- ↵A good review about fluoroscopic and angiographic heart anatomy for catheter ablation mapping and ablation of arrhythmias.
- ↵
- ↵This article shows the architecture of the human sinus node to facilitate understanding of mapping and ablative procedures in its vicinity.
- ↵
- ↵This study provides important morphological details for a better understanding of the structure of the right atrial cavo-tricuspid isthmus.
- ↵
- ↵
- ↵This is an interesting study about the gross arrangement of the principal muscular bundles of the atria to provide a morphologic basis for atrial conduction and potential substrates of arrhythmias.
- ↵
- ↵This article re-examines the anatomy of the left atrium from the viewpoint of an electrophysiologist.
- ↵
- ↵This study reveals the characteristics of normal pulmonary veins so as to provide more information relevant to radiofrequency ablation.
- ↵This study aims to provide an insight into the structure of the left lateral atrial ridge and associated structures in this region such as the oblique vein of Marshall and vegetative nerves.
- ↵
- ↵
- ↵
- ↵This review explores the anatomy of the pericardial space and the anatomic variants that may be encountered in this approach to the heart.
- ↵This study reveals the characteristics of the non-uniform thickness of the posterior left atrial wall and the variable fibro-fatty layer between the wall and the oesophagus which are risk factors that must be considered during the ablation procedure.
- ↵This study clarifies the spatial relationships between the phrenic nerves and important cardiac structures which is essential to reduce risks during epicardial and endocardial catheter ablation.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online references
Footnotes
-
Contributors Hospital Universitario Quirón-Madrid, Universidad de Extremadura.
-
Competing interests In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article. The authors have no competing interests.
-
Patient consent Obtained.
-
Ethics approval Bioethics and Biosafety Committee of the University of Extremadura (Badajoz, Spain).
-
Provenance and peer review Commissioned; externally peer reviewed.