Article Text

Statistics from Altmetric.com
Learning objectives
Describe the prevalence and predictors of neurocognitive and psychosocial impairment among adults with congenital heart disease.
Improve one’s ability to identify and address neurocognitive and psychosocial impairment in the clinical setting.
Summarise the potential role of mental health professionals in the care of adults with congenital heart disease.
Introduction
In 1964, Glaser recognised that, ‘Despite benefits derived from these remarkable therapeutic gains, children with congenital heart disease face many difficulties in their efforts toward social and emotional adjustment.’1 In 1981, Doucet wrote, ‘The impact of congenital heart disease on the individual would not be limited to the physiological alteration in the heart’s functioning but would affect the whole individual.’2 Recognition of the broader lifestyle implications of congenital heart disease (CHD) for both children and adults is thus not a modern concept. However, what is unique to the current era of CHD care in developed countries is that over 90% of infants born with CHD survive to adulthood, with the number of adults living with CHD now far surpassing the number of children.3 This demands that we expand our definition of successful adult CHD (ACHD) outcomes to include good quality of life, including the best possible neurocognitive and psychosocial functioning, and target our clinical efforts accordingly.
Although neurocognitive and psychosocial outcomes among adults with CHD are often considered independently, this silo-oriented approach ignores their reciprocal interplay. For example, neurocognitive, academic and occupational functioning can be adversely affected if a person is struggling with anxiety or depression. Similarly, neuropsychological deficits can adversely affect social development, impairing one’s ability to establish and sustain satisfying relationships in adulthood. In addition, one cannot fully appreciate adult outcomes without considering their origins in childhood and adolescence. In this review, we thus apply a developmental lifespan perspective to better understand neurocognitive and psychosocial outcomes of adults with CHD. We also propose opportunities and strategies for ACHD providers and programmes to enhance meaningful patient outcomes.
Neurocognitive outcomes
Paediatric outcomes that typically carry through to adulthood
Although most children with CHD demonstrate neurocognitive development within the normal range, they are at increased risk of neurodevelopmental deficits, with both risk and severity increasing with disease complexity.4 These deficits primarily involve the domains of behaviour, language, speech, attention and executive functioning.4 Perioperative factors are not clearly linked with outcomes,5 and abnormal brain development predates surgery.6 Length of hospital stay and socioeconomic status are two key factors associated with poorer neurodevelopmental outcomes.7 Outcomes tend to be more variable in children with CHD than in children without CHD, likely due to the increased frequency of genetic syndromes, most notably 22q11.2 deletion syndrome, and adverse events such as stroke and seizures.4
The frequency and severity of neurodevelopmental difficulties tend to increase as children with CHD age, especially during middle and later primary school years. This is likely the result of increasing demands for self-regulation and other executive skills, especially in the school setting. Problems that might emerge include time management, planning and organising, seeing the ‘big picture’ without getting lost in details, cognitive flexibility (eg, multitasking), working memory, impulse control and anticipating future consequences. In addition, children with CHD might demonstrate difficulties with fine motor skills (eg, mastering penmanship), visual-spatial skills, attention (distractibility), processing speed and higher order language skills.4 Impaired executive functioning, including attention-deficit/hyperactivity, is more common among patients with more severe forms of CHD, such as single-ventricle physiology.8 9 A recent systematic review of 100 methodologically sound studies investigating developmental outcomes of infants, children and adolescents with complex CHD demonstrated poorer outcomes among patients with single-ventricle CHD.5 Because of these potentially additive and interactive neurodevelopmental challenges, half of children with complex CHD require one or more remedial academic services (eg, special education, tutoring, early intervention, occupational therapy).10
Neurocognitive challenges of adolescence and early adulthood
A scientific statement from the American Heart Association outlining best practices for the management of adolescents transitioning to ACHD care underscores the fact that neurodevelopmental deficits can affect patients’ capabilities for self-management skills that are required to eventually assume maximal responsibility for healthcare management.11 Many of the neurodevelopmental deficits first detected in childhood are unsurprisingly also present in adolescence and adulthood, often becoming more pronounced. A meta-analysis of 18 cohorts of adolescents and adults with CHD (excluding individuals with chromosomal or genetic abnormalities) found that although general intelligence was comparable to controls when collapsed across defect complexity, deficits were consistently observed in specific cognitive domains including psychomotor skills, working memory, processing speed and attention.12
Individuals with CHD tend to have higher rates of autism spectrum disorder and poorer social cognition skills than their peers.13–15 Social cognition skills enable one to ‘read’ the thoughts and emotions of other people, and individuals without these abilities can have difficulty establishing and sustaining satisfying social relationships.16 This demonstrates the important interplay between neurocognitive and psychosocial functioning. Conversations among adolescent peers are fast paced and affect-laden, and language tends to be pragmatically complex (involving sarcasm, innuendo, insult, cajoling, deception and other indirect communications). Someone with deficits in cognitive processing, executive functions (specifically in working memory and cognitive flexibility), emotion recognition and pragmatic language skills would find such interactions challenging, potentially increasing the risk of anxiety or depression. Such challenges would likely persist into adulthood, and deficits in theory of mind (ie, the ability to attribute mental states to others and ourselves) have indeed been reported in adults with CHD, even those with more simple forms of the disease.13 17
Neurocognitive presentation in adulthood
Two important patterns observed in children have also been noted in adults, namely the increased likelihood of deficits in executive functions and poorer neurocognitive outcomes in those with more complex disease.12 18–21 Researchers have begun using imaging techniques to better understand these deficits. Structural abnormalities on brain MRI (eg, white matter lesions, global atrophy, small hippocampal volumes) are more common among adults with CHD and associations with intellectual outcomes are being explored.22 23 A systematic review of 14 studies concluded that structural brain abnormalities were almost eight times higher among adolescents and adults with CHD compared with comparative samples.24 A recent study of 66 adults with CHD of simple complexity (isolated atrial or ventricular septal defects), however, did not detect major structural brain abnormalities compared with healthy matched peers.17
In addition to deficits carried forward from childhood, there are additional risk factors for cognitive dysfunctions that typically emerge in adulthood. Factors on this list are not mutually exclusive and include arrhythmias, heart failure, hypertension, coronary artery disease and diabetes mellitus.6 25 These comorbidities place individuals at risk for reduced cerebral blood flow, reduced brain volume and dementia.6 The observed prevalence of cognitive impairment among 26 studies of adults with heart failure due to acquired heart disease was 43%26 and we might anticipate a similarly high risk among individuals with heart failure associated with CHD. In a Danish cohort study, adults with CHD were observed to have an increased risk of dementia, particularly for early-onset dementia presenting before the age of 65, compared with the general population.27 Adults with CHD have been described as ‘vulnerable hosts who are potentially susceptible to further cognitive insults’.25
Neurocognitive impairments in adults with CHD have significant ramifications for health outcomes and quality of life. With regard to cardiac morbidity and mortality, optimal outcomes demand that patients understand, agree with the importance and adhere to recommended health behaviours. Further, the complexity of disease regimens tends to increase as health status worsens. For example, adults with CHD and advanced heart failure are typically asked to attend more frequent clinic appointments, restrict fluids and sodium, adhere to complicated medication regimens and be vigilant to symptoms (such as rapid weight gain) that warrant urgent medical attention. Full adherence may be challenging in the context of even mild cognitive impairment. The broader potential impact of neurocognitive deficits on quality of life, particularly achievement of milestones associated with independent adulthood, must also be considered. For example, poorer performance on tests of executive functions has been observed among patients receiving disability.19 Patients with complex disease have lower educational attainment and higher unemployment.28 Lack of employment, in turn, has been associated with poorer quality of life and more symptoms of depression and anxiety in an international study of approximately 4000 adults with CHD.29 Among adults with CHD, poorer executive functions have been associated with less effective coping strategies and greater emotional distress.30 31 In summary, adults with CHD face an increased risk of neurocognitive impairment with aetiological factors that may present at any point across the lifespan and carry broad implications for their lives across physical, social and psychological domains.
Psychosocial outcomes
Paediatric outcomes that carry through to adulthood
Like neurocognitive challenges, the behavioural difficulties of children with CHD tend to become more apparent with age. By school age, both parent and teacher ratings suggest elevated risk of children’s behaviour being problematic, particularly in terms of internalising behaviours (namely anxiety and depression).32 By the time children with CHD reach adolescence, clinicians rate them as having poorer global psychosocial status, with a substantial subgroup, especially those with more complex disease, manifesting ratings in the range of clinical concern.33 A systematic review and meta-analysis of 16 studies examining psychosocial outcomes in children and adolescents with severe CHD concluded that 25% of participants had internalising behavioural problems.34 Among adolescents with single-ventricle CHD with Fontan physiology, the frequency of any psychiatric disorder may be as high as 65%.9 Recommendations from the Association for European Paediatric and Congenital Cardiology advocate for a holistic and family-centred approach to the care of children and adolescents with CHD.35
Psychological distress in adulthood
In the ACHD setting, there is now widespread acceptance of the psychosocial impact of living with a lifelong cardiac condition. In a review of 20 articles published between 1991 and 2017, the prevalence of depression among adults with CHD varied widely, ranging from 6% to 69%.36 How researchers assess depression appears to be critical for the interpretation of results. A meta-analysis of 22 studies restricted to outcomes assessed by self-report symptom surveys concluded that adolescents and adults with CHD did not differ from healthy peers in terms of emotional functioning, although significant heterogeneity was observed.37 In contrast, North American studies that used clinical interviews reported an elevated risk of mood or anxiety disorders in adults with CHD, with approximately one-third meeting diagnostic criteria.38–40 It is noteworthy that the sample in one of these studies was limited to ‘well adjusted’ patients without symptoms of depression or anxiety known to their providers, yet 8 of 22 interviewed participants were assigned a psychiatric diagnosis.38 This study was published in 2003 and it is unknown whether there has been subsequent improvement in ACHD providers’ ability to detect clinically significant psychological distress. The use of structured diagnostic interviews has also demonstrated higher lifetime prevalence of depression and anxiety in other countries. For example, a study of 67 adults with dextro-transposition of the great arteries in France observed a lifetime prevalence of depression of 43% and of anxiety disorders of 54%.20 Similarly, structured interviews administered to 150 adults with CHD in Germany revealed a prevalence of psychiatric disorders of 48%, with mood and anxiety disorders having similar prevalence rates.41 Negative psychological outcomes among adults with CHD are not ubiquitous, however, as positive outcomes have been observed among patients living in the Netherlands.42
Although the traditional psychological focus of cardiology has been depression, this perspective is too limiting and does not capture the psychological experience of many individuals living with heart disease. Providers caring for adults with CHD should be aware of the elevated risk of anxiety, post-traumatic stress disorder and, among certain patient cohorts, psychotic disorders. Among adults with CHD, elevated anxiety symptoms seem to be more common than depression symptoms among studies of clinic outpatients as well as adults presenting for psychological care.43 44 In another study, approximately one in five patients reported elevated symptoms of post-traumatic stress disorder.45 Although beyond the scope of this review, there are certain subgroups of adults with CHD that are at elevated risk of significant psychiatric impairment. For example, patients with conotruncal heart defects have a higher prevalence of 22q11.2 deletion syndrome, which carries an increased risk of significant mental illness including schizophrenia.46
Biopsychosocial framework
Within a biopsychosocial framework, the potential challenges that adults with CHD face in achieving well-being can be categorised as biomedical (eg, repeat surgical and catheter interventions, implanted devices, decline in health status), psychological (eg, self-esteem, identity formation) and social (eg, feeling different, social isolation, and family planning and employment considerations).47 48 The interplay between social and psychological well-being was demonstrated by the results of one study in which loneliness and social anxiety were stronger predictors of mood and anxiety symptoms than lesion complexity.40 Findings are inconsistent with regard to the impact of age, sex and disease severity on psychological functioning.48 Objective health markers may be less relevant than subjective functional health status in determining an individual’s psychological well-being and quality of life.29 40
By its very definition, psychological distress is unwelcome and, depending on severity and duration, might warrant clinical intervention. Moreover, there is emerging evidence that psychological factors may influence medical outcomes among adults with CHD. Specifically, elevated psychological distress and/or the presence of psychiatric disorders have been associated with shorter event-free survival, higher healthcare utilisation including more outpatient visits, more emergency department visits, more hospitalisations and more costly hospital admissions.49–51 Although we do not currently have evidence that psychological interventions can improve medical outcomes, these studies illustrate the complexity of the bidirectional relationship between psychosocial and medical factors.
Clinical opportunities in ACHD
Awareness of the psychosocial implications of CHD dates back over 50 years and has subsequently been supported by decades of empirical study. Combined with notable improvements in morbidity and mortality, this awareness provides the impetus for expanding the definition of successful CHD outcomes. Within the current era of comprehensive ACHD care, we now have the opportunity to optimise neurocognitive and psychosocial well-being through coordinated efforts to identify and treat impairment in the clinical setting. Such efforts require close collaboration between ACHD physicians, nurses, advanced practice providers and mental health professionals.
Strategies to improve the identification of neurocognitive impairment
Although many paediatric programmes have established cardiac neurodevelopmental follow-up clinics,4 routine neurocognitive assessment remains rare in the adult setting. One ACHD clinic began screening patients for neurocognitive impairment using a 10-item self-report measure that assessed perceived competence in several domains (including attention, memory and executive functioning).52 Of 337 patients who were screened, 116 (34%) reported significant neurocognitive deficits as determined by a scoring system developed by the researchers. Interestingly, most of these 116 patients who were offered formal neurocognitive testing did not take advantage of this option, typically declining (n=46) or not arriving for scheduled assessments (n=40).
In the absence of screening or formal neuropsychological assessment, the importance of addressing this matter within the context of routine ACHD clinical encounters becomes even greater. The top half of table 1 offers a list of questions that ACHD providers might consider in the clinical setting to obtain a broad sense of neurocognitive functioning. This list includes questions pertaining to education and employment history, which provide general insight into neurocognitive functioning across the lifespan. For example, providers can inquire whether patients have previously been diagnosed with a learning disability or received remedial academic services. Ideally, the paediatric care team would communicate such information, if known, to the ACHD team at the time of transfer of care. Following transfer to ACHD care, providers can inquire about a patient’s ability to complete postsecondary education and/or sustain employment. Table 1 also includes examples of questions pertaining to health self-management skills, which generate insight into current health-specific cognitive abilities. During ACHD follow-up visits, providers are encouraged to be mindful of risk factors for cognitive impairment that typically present in adulthood (eg, heart failure) and inquire about cognitive changes observed by patients or their family members.
Strategies for identifying and addressing neurocognitive impairment
Strategies to improve the identification of significant psychological distress
Awareness of the elevated prevalence of clinically significant psychological distress often triggers calls for routine screening of adults with CHD. However, strong evidence to support the efficacy of routine depression screening in cardiology is lacking, and this practice is not without potential risk (eg, false positives).53 There are also logistical challenges to screening that entail making important decisions about the following: (1) the psychological symptoms/disorders for which to screen (eg, depression, anxiety, post-traumatic stress disorder, or others), (2) the most appropriate screening measure(s) and methods (eg, pen and paper vs electronic), (3) which member(s) of the ACHD team will be responsible for administering surveys, reviewing results and interpreting results with patients, (4) how to integrate results within the medical record, and (5) how follow-up services will be coordinated. Given that the integration of mental health professionals within ACHD programmes is currently uncommon, questions about resource allocation are critical. For example, when faced with a decision between psychological screening of all patients versus psychological treatment of patients identified as having significant emotional distress, ACHD programmes might prioritise the latter.
Challenges in routine screening using self-report measures do not eliminate the clinical aim of identifying psychosocial impairment that warrants clinical attention. The top half of table 2 offers a list of questions that may foster awareness and encourage disclosure and identification of significant psychosocial distress in clinical settings. This list includes questions to discern psychological well-being as well as patients’ ways of managing psychological distress (including personal coping strategies and current or past mental health treatment). American ACHD guidelines propose asking ‘simple questions’ about anxiety and depression during clinical encounters.54 Programmes are encouraged to foster a culture of awareness among all stakeholders (patients, family members and providers) regarding the potential psychosocial implications of CHD, thus encouraging open inquiry and discussion during both outpatient and inpatient settings. This dialogue is ideally ongoing, as biopsychosocial challenges impacting psychological well-being as well as coping skills may evolve over time.55
Strategies for identifying and addressing psychological distress
Strategies targeting educational, occupational and self-management outcomes
Consistent with a developmental lifespan perspective, the aim in the paediatric setting can be to develop a proactive approach to mental health that may reduce the incidence and/or impact of neurocognitive, emotional and social difficulties in adulthood. In the adult setting, the goal is to optimise neurocognitive and psychosocial outcomes through collaboration with mental health professionals. Strategies to promote achievement of realistic educational and occupational goals as well as health self-management skills are offered in the bottom half of table 1. Within the ACHD setting, patients with known neurocognitive deficits can be directed towards available services for education (eg, academic disability resource centres) and employment (eg, job training or vocational rehabilitation).25 52 It is also important to develop strategies for patient education and self-management skills that are commensurate with and individualised to patients’ cognitive abilities.
Strategies targeting psychosocial outcomes
Unfortunately, most adults with CHD who have mood and/or anxiety disorders do not receive mental health treatment.38–41 As described earlier, ACHD programmes are encouraged to create an environment that fosters discussion of patients’ psychological challenges and coping abilities. The bottom half of table 2 offers examples of statements that non-mental health providers may consider in order to destigmatise psychological distress as well as strategies to promote mental well-being.
There are different approaches to the provision of mental healthcare to adults with CHD. The integration of mental health professionals (eg, psychologists, psychiatrists, counsellors, licensed clinical social workers) within ACHD programmes is clearly optimal as this approach demonstrates a programme’s strong commitment to interdisciplinary psychosocial care. However, for many programmes, linking with external mental health providers (within the same hospital or the local community) may currently be more feasible. At a minimum, ACHD programmes should establish appropriate mechanisms for follow-up for patients who report or exhibit significant emotional distress. Box 1 lists reasons that might prompt referral to a mental health professional with particular expertise in health psychology rather than a general practitioner.
Prompts for referral to a mental health professional with expertise in health psychology (when available)
Congenital heart disease (CHD) (diagnosis or treatment) contributing to anxiety or depressed mood.
Heart-focused worry in the context of otherwise positive psychological adaptation.
Difficulty coping with CHD or declining health status.
Difficulty with the transition from paediatric to adult care.
Difficulty with adherence (eg, medications, medical appointments).
Challenges communicating effectively with healthcare providers.
Body image concerns due to CHD or its treatment.
Challenges with social relationships (eg, difficulty keeping up with peers or talking about illness with family or friends).
Need for support with decision-making related to cardiovascular care (eg, implantable cardioverter-defibrillator or ventricular assist device implantation).
Difficulty adjusting to implanted cardiac devices.
Preparation for surgery/catheterisation.
Significant change in cognitive functioning (eg, following sudden cardiac arrest).
Concerns regarding future health expectations (mortality, advance care planning and/or end-of-life care).
Mental health interventions include individual and/or group therapy, pharmacotherapy and peer support. In a survey of adults with CHD who reported preferences for future mental health treatment, 41% chose psychotherapy, 9% preferred pharmacotherapy and 34% indicated that either modality would be acceptable.56 Adults with CHD have previously expressed strong interest in opportunities to interact with other adults with CHD, to provide and receive peer support and to receive psychosocial treatment in small groups.56 57 Potential psychotherapeutic interventions include cognitive–behavioural therapy, mindfulness-based interventions and interpersonal therapy.48 A feasibility study demonstrated that it is possible to execute a randomised controlled trial of a cognitive–behavioural psychosocial intervention for adults with CHD, although practical barriers to participation in a group (eg, transportation, scheduling) must be addressed.58 Given the relationship between executive functions and coping in adults with CHD, patients with deficits in executive skills might benefit from additional assistance when learning cognitive–behavioural coping strategies.30 With regard to psychotropic medications, selective serotonin reuptake inhibitors are the recommended class of antidepressant medications for adults with cardiovascular disease,59 although no studies have been conducted in patients with ACHD.
Conclusions
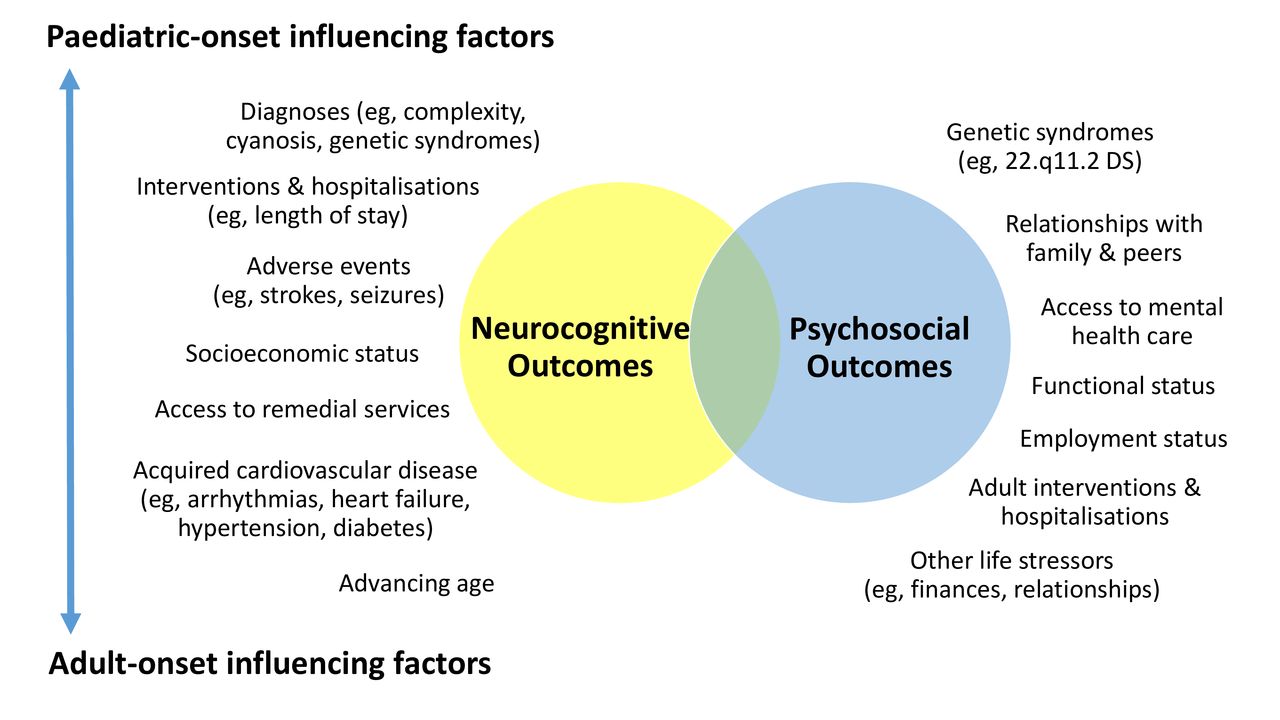
As a result of significant advances in diagnosis and surgical/catheter interventions, CHD teams now have the collective opportunity to achieve outcomes beyond improved survival and life expectancy. The complex interplay between medical, neurocognitive and psychosocial functioning across the lifespan of individuals with CHD demands interdisciplinary care as well as seamless collaboration between paediatric and adult providers. Figure 1 depicts the relationship between neurocognitive and psychosocial outcomes and identifies paediatric-onset and adult-onset factors known to influence outcomes. Awareness of the impact of CHD on patients’ lifestyles and well-being has existed for over half a century and in more recent decades, researchers have focused on elucidating the prevalence and predictors of neurocognitive impairment and psychosocial distress. Awareness of the psychosocial impact of CHD without action, however, is no longer sufficient. Access to mental healthcare and the continued development and evaluation of psychological interventions are natural and critical next steps in ACHD care. Sustainable models for psychosocial care integrated within ACHD programmes are unlikely to develop without strong advocacy from providers, patients and families. Prioritisation by programmatic and institutional leaders and decision makers is also essential.

{kind=link}
Paediatric-onset and adult-onset factors influencing neurocognitive and psychosocial outcomes.
Key messages
A developmental lifespan perspective is required in order to understand neurocognitive and psychosocial outcomes of adults with congenital heart disease.
In addition to neurodevelopmental deficits that might be carried over from paediatrics, individuals with congenital heart disease face additional risk factors for cognitive dysfunction in adulthood.
Most, but not all studies that use clinical interview methodology suggest that adults with congenital heart disease are at risk of clinically significant depression and anxiety.
There is emerging evidence that psychological factors may influence medical outcomes among adults with congenital heart disease.
Adult congenital heart disease programmes have the opportunity to optimise neurocognitive and psychosocial well-being through coordinated efforts to identify and treat impairment in the clinical setting and collaborate with mental health professionals.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the 'Take the Test' link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
References
Footnotes
Contributors Both authors contributed to the preparation of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.
Data availability statement There are no data in this work.
Author note References which include a * are considered to be key references