Article Text

Statistics from Altmetric.com
Several prior studies have shown that patients with diabetes mellitus have worse in-hospital outcomes compared to non-diabetic patients when admitted for an acute myocardial infarction (MI).1,2 Few studies have examined this same issue among patients admitted across the entire spectrum of acute coronary syndromes (ACS) (unstable angina, non-ST elevation MI, ST elevation MI).3,4 Since patients admitted with these diagnoses make up a large proportion of admissions to cardiology services and diabetic patients represent a sizeable portion of these patients, investigation of this cohort is clinically pertinent.
METHODS
In the present study, we analysed patients with and without diabetes, with the goal of systematically examining similarities and differences in presentation, management, and outcomes when admitted for ACS. We studied 1951 consecutive patients who were admitted to the University of Michigan Medical Center from 27 December 1998 to 16 October 2002 with a diagnosis of ACS. The protocol was approved by the institutional review board at the University of Michigan and informed consent was obtained from all patients. Diabetes was defined as a known history of type I or type II diabetes mellitus treated with diet, oral glucose lowering agents, or insulin. Patients utilising insulin for the management of their diabetes before admission were included in the insulin treated diabetic subset. Multivariate logistic regression was used to estimate adjusted odds of adverse events for patients with diabetes relative to patients without diabetes. All analyses were performed using SAS 8.2 (SAS Institute, Cary, North Carolina, USA).
RESULTS
Of the 1951 patients who were admitted for an ACS, 598 (31%) had a previous diagnosis of diabetes mellitus. Mean (SD) age (63.7 (12.3) v 63.3 (14.1) years, p = 0.53), and sex (62.2% v 65.9% male, respectively, p = 0.11) were similar between patients with and without diabetes. Forty nine per cent of the diabetic patients were identified as utilising insulin to manage their diabetes. Of the 598 patients with diabetes, approximately 72% were diagnosed with an acute MI. Diabetic patients were less likely to present with ST elevation MI and more likely to present with non-ST elevation MI compared to non-diabetic patients. Diabetic patients had higher frequencies of hyperlipidaemia, hypertension, obesity, heart failure, and previous MI and were more likely to have a prior diagnosis of renal insufficiency or end stage renal disease, peripheral vascular disease, and prior history of stroke or transient ischaemic attack.
Patients with and without diabetes were equally likely to present with dyspnoea, diaphoresis, or left arm pain. However, 87% of non-diabetic patients versus 81% of diabetic patients presented with chest pain, a small but significant difference (p < 0.01). ST segment changes were less common in diabetic patients but left bundle branch block pattern was seen more often. The frequency of cardiac enzyme elevations was not different from that of the non-diabetic patients.
Diabetic patients and non-diabetic patients received similar in-hospital management, but with important differences. Both groups received aspirin, β blockers, nitrates, and lipid lowering agents equally; however, diabetic patients were less likely to be treated with thrombolytic drugs and were less likely to undergo coronary angiography and percutaneous coronary interventions.
The rates of individual in-hospital complications were significantly increased in the diabetic patients versus non-diabetic patients. Diabetic patients experienced more heart failure, pulmonary oedema, and renal failure while in the hospital. In-hospital mortality was increased by 90% in patients with diabetes (7.3% v 4.0%, p = 0.0017; odds ratio (OR) 1.91, 95% confidence interval (CI) 1.27 to 2.88).
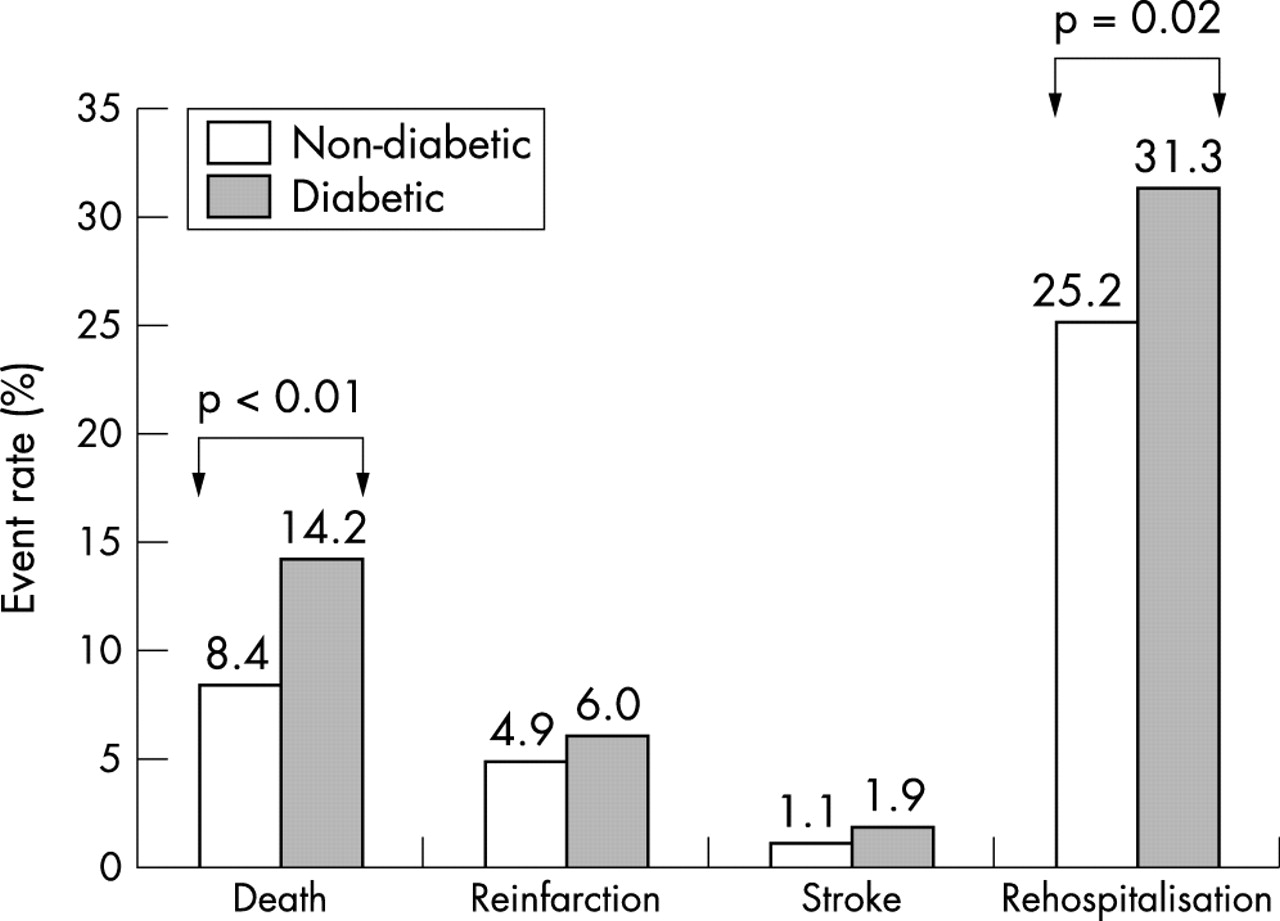
The relation of diabetes mellitus with worse outcome persisted six months after discharge. Significantly more diabetic patients died (14.2% v 8.4%, p = 0.0012) or were rehospitalised for heart disease (31.3% v 25.2%, p = 0.02) in the six months following their hospitalisation for ACS (fig 1). Rates of recurrent or new MI were not significantly different. The difference in mortality (in-hospital mortality plus mortality at six months) persisted when controlling for age, sex, body mass index, smoking, and histories of hypertension, hyperlipidaemia, heart failure, MI, renal failure, and angina (OR 1.55, 95% CI 1.15 to 2.07; p < 0.01) (table 1). Diabetes also conferred a trend towards higher risk of stroke after adjustment for co-morbidities and was associated with a reduced likelihood of recurrent angina.
Univariate and multivariate risk adjusted odds ratios for adverse in-hospital clinical outcomes in diabetic patients presenting with ACS

{kind=link}
Clinical outcome in diabetic patients presenting with ACS compared to non-diabetic patients.
There was a significant interaction with diabetes and age for mortality (p = 0.01 for the interaction), with higher mortality noted for younger patients with diabetes. The odds ratio for mortality in diabetic patients < 55 years compared to non-diabetic patients < 55 years was 6.04 (95% CI 2.25 to 16.18, p = 0.0003) and for individuals > 55 years the odds ratio was 1.40 (95% CI 0.88 to 2.24, p = 0.15). When comparing insulin treated diabetes mellitus patients with non-insulin treated diabetes mellitus patients, the insulin treated diabetic patients had increased in-hospital mortality and this difference was also significant at six months follow up. Regarding total mortality, 18.6% of insulin treated diabetic patients died in the hospital or by six months versus 11.7% of the non-insulin treated diabetic patients and 8.4% of the patients without diabetes (p = 0.001).
DISCUSSION
Our study shows diabetes mellitus to be a strong independent predictor of adverse outcomes for patients admitted across the entire spectrum of ACS. The risk seems to be accentuated in patients with insulin treated, compared to non-insulin treated, diabetes mellitus and in younger individuals. The analysis also revealed a significant interaction of diabetes with age, suggesting that diabetes may be a particularly important risk factor in younger patients. This is supported by a recent study which demonstrated that diabetes is a major risk factor for adverse events in young patients with atherosclerosis.5
In conclusion, this study demonstrates that diabetes confers increased mortality for patients admitted for the entire spectrum of ACS, particularly in insulin treated patients. Not only did our diabetic patient cohort carry a heavier burden of co-morbidities, but diabetes itself was shown to be an independent predictor of death. These data should serve as a signal to us to be more aggressive in identifying and treating the other atherosclerosis risk factors that ultimately lead patients with diabetes to present with coronary events.
Acknowledgments
This study was supported in part by the Mardigian Foundation Grant.