Article Text

Abstract
Nutrition has a central role in both primary and secondary prevention of cardiovascular disease yet only relatively recently has food been regarded as a treatment, rather than as an adjunct to established medical and pharmacotherapy. As a field of research, nutrition science is constantly evolving making it difficult for patients and practitioners to ascertain best practice. This is compounded further by the inherent difficulties in performing double-blind randomised controlled trials. This paper covers dietary patterns that are associated with improved cardiovascular outcomes, including the Mediterranean Diet but also low-carbohydrate diets and the potential issues encountered with their implementation. We suggest there must be a refocus away from macronutrients and consideration of whole foods when advising individuals. This approach is fundamental to practice, as clinical guidelines have focused on macronutrients without necessarily considering their source, and ultimately people consume foods containing multiple nutrients. The inclusion of food-based recommendations aids the practitioner to help the patient make genuine and meaningful changes in their diet. We advocate that the cardioprotective diet constructed around the traditional Mediterranean eating pattern (based around vegetables and fruits, nuts, legumes, and unrefined cereals, with modest amounts of fish and shellfish, and fermented dairy products) is still important. However, there are other approaches that can be tried, including low-carbohydrate diets. We encourage practitioners to adopt a flexible dietary approach, being mindful of patient preferences and other comorbidities that may necessitate deviations away from established advice, and advocate for more dietitians in this field to guide the multi-professional team.
- cardiac rehabilitation
- hypertension
- lipoproteins and hyperlipidaemia
- metabolic syndrome
- diabetes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
There are multiple modifiable risk factors for cardiovascular disease (CVD), many of which are modifiable via changes in diet and physical activity. This combination is widely recognised in clinical guidelines as being important in both primary and secondary prevention,1–3 and nutritional education is an important element of cardiac rehabilitation (CR). However, the area of nutrition is frequently over complicated with conflicting information. Such an example is salt, with recent evidence suggesting the benefit of salt restriction is greatest in those already with hypertension (HTN),4 and that both low and high intake may be associated with increased mortality.5
Patients with cardiac disease are becoming increasingly more complex due to the number of comorbidities present. Data from the National Audit of Cardiac Rehabilitation (NACR) show HTN to be the most common comorbidity (49.9%), followed by hypercholesterolaemia/dyslipidaemia (31.7%) and then diabetes (24.5%).6 Poor diet is a significant modifiable risk factor in these comorbidities, and all outcomes reported by the NACR could likely be improved with increased emphasis on addressing lifestyle (nutrition and exercise).
The Diet working group was established by British Association for Cardiovascular Prevention and Rehabilitation (BACPR) and was actioned to provide a guide through current controversies in cardiovascular nutrition, in addition to signposting researchers to current gaps in evidence. The group sought views from professionals working in the area of CR and aims to provide specific recommendations to answer the many common questions encountered by healthcare professionals working in this field. This paper reviews both macronutrients and the key food groups healthcare professionals sought clarity on.
The objectives of this paper are to review the area of cardiovascular nutrition and provide recommendations for practitioners to help patients make healthy eating decisions. We also aim to identify current gaps in evidence and suggestions for future research.
Macronutrients
Protein
Summary messages regarding dietary protein are presented in table 1. Detailed study7–13 analysis examining protein intake and CVD are presented in online supplementary table 1.
Supplemental material
Protein
There is a long-standing argument that high protein intakes lead to renal failure with a recent observational study suggesting that increased protein intake post-myocardial infarction (MI) was associated with a greater decline in renal function7 and increased risk of mortality.8 Of interest, dairy or plant protein sources showed a much weaker association when compared with animal protein, and the relationship between protein and outcome variables was stronger in those with predisposing disease, for example, diabetes. This indicates that the source of dietary protein may be important to consider. Indeed, randomised controlled trials show that the quality of meat (in addition to the whole diet) is likely to be an important factor to consider in explaining this relationship, with evidence suggesting that the addition of lean red meat to an already low saturated fat cardioprotective diet does not impact negatively on blood lipids.9 The saturated fat content of the comparison diet10 may be an additional piece of the puzzle in explaining the impact dietary protein (and its source) has on cardiovascular health.11
Protein provides the main components for muscle synthesis and consensus opinion suggests that protein intakes should be higher in the elderly12 with intakes up to 1.5 g/kg/d being shown to improve body composition in an elderly, frail population.13 Collectively, these studies highlight an important role for protein in cardiovascular health, especially when considering (a) source (animal vs plant); (b) quality and (c) overall diet quality.
Carbohydrates
Summary messages regarding dietary carbohydrate are presented in table 2. Detailed study14–19 analysis examining carbohydrate intake and CVD are presented in online supplementary table 1.
Carbohydrate
The Prospective Urban Rural Epidemiology study raised carbohydrates to the forefront of cardiovascular health with headline data showing higher carbohydrate intake was associated with increased all-cause and cardiovascular (CV) mortality.14 However, recent meta-analyses examining the association between carbohydrate intake and cardiovascular health have suggested a U-shaped relationship between carbohydrate and all-cause mortality, specifically in those consuming a low-carbohydrate diet higher in animal protein and fat.15 16
Prospective cohort studies have shown fibre intake to be inversely associated with reduced cardiovascular and all-cause mortality post-MI.17 In this study,17 only cereal fibre was significantly associated with a reduction in cardiovascular and all-cause mortality in both men and women. One of the most prominent sources of cereal fibre is whole grain, and whole grain is frequently cited as being beneficial for health11 18; however, there is disparity between meta-analyses of cohort studies and results from randomised controlled trials.19 Such discrepancy between this and prospective studies likely highlights the importance of adequately defining whole grain, and taking a whole diet approach when considering cardioprotective foods.
Fats
Summary messages regarding dietary fat are presented in table 3. Detailed study20–24 analysis examining fat intake and CVD are presented in online supplementary table 1.
Fat
The correct balance of dietary fats is a key to cardiovascular health; however, as with carbohydrates and protein types, sources and amounts have made determining effects difficult. Saturated fat has long been suggested to be harmful for cardiovascular health; however, a recent meta-analysis20 suggested that reducing saturated fat did not seem to effect total mortality or CVD mortality. However, a reduction in combined cardiovascular events of 17% was shown with a reduction in saturated fat. Greater decreases in events were seen for studies that replaced saturated fat with polyunsatured fats when compared with monounsaturated fats, carbohydrate or protein.20 Thus, it would appear reducing saturated fat and replacement with unsaturated fat conveys the greatest cardiovascular benefit, not necessarily reducing saturated fat and replacing with refined carbohydrate, and some of this effect may be modified by where the saturated fat is found that is, dairy versus processed baked goods.
Increased trans fat intake is positively associated with total mortality, along with animal monounsaturated fats, alpha linolenic acid and arachidonic acid.21 In this same study, marine n3 polyunsaturated fat and replacement of saturated fat with plant monounsaturated fat were associated with lower total and CVD mortality. This latter study acknowledges the subtypes of fat such as n3 (alpha linolenic acid, eicosapentaenoic acid and docosahexaenoic acid) and n6 fatty acids (linoleic acid and gamma-linoleic acid). Indeed, n6 fatty acids have been shown to reduce risk of MI, as well as reducing total cholesterol (TC), with these findings possibly relating to both baseline n6 intake and dose of n6 provided.22 This latter point is similar to observations made in the most recent analysis of fish oil supplements and cardiovascular health. This analysis indicated no benefit from supplementation on reducing fatal coronary heart disease (CHD) or any CVD in people with or at high risk of CVD,23 primarily due to the low dose of eicosapentaenoic acid and docosahexaenoic acid used in the included studies (226 to 1800 mg/day and 0 to 1700 mg/day, respectively). These null results contrast substantially with the positive effects seen with the Reduction of Cardiovascular Events with Icosapent Ethyl–Intervention Trial utilising a highly purified form of eicosapentaenoic acid (4 g/day).24 Further research into specific fat replacements for saturated fat is warranted and it is unclear whether there is additional benefit to maintaining a lower saturated fat diet while on lipid-lowering treatment. As with protein and carbohydrate, the source of the nutrient (ie, food) matters.
Foods and food groups
Detailed information considering food and food groups are shown in online supplementary table 2.
Fruits and vegetables
The grouping of fruits together with vegetables is inaccurate, similarly to the grouping of red and processed meat. This ignores distinct differences between fruits and vegetables in terms of their nutrient profile, and hence their association with disease. Fruits and vegetables high in nutrients are hypothesised to be cardioprotective and have consistently been associated with reduced CVD.25 Hence, fruits and vegetables are cornerstones of cardioprotective dietary patterns (eg, dietary approaches to stop hypertension (DASH), Mediterranean) and dietary guidelines ubiquitously recommend them.1–3
However, a systematic review and meta-analysis26 is notable whereby there was an inverse association between both reported dietary intake and blood concentrations of vitamin C, carotenoids and α-tocopherol (markers of fruit and vegetable intake) with risk of CVD, and all-cause mortality. Interestingly, inverse associations between disease/mortality endpoints were stronger for measured biomarkers than for reported dietary intake suggesting that the methodology used to collect this information may be a unreliable.26 Multiple studies have shown fruits and vegetables to be consistently associated with reduced CHD and stroke incidence, HTN, and CVD mortality.26 27 However, debate exists on the physical amounts to be consumed, with some suggestions of CHD benefit over 400 g/day26 and others showing little further benefit of over 300 g/day.27 Existing randomised controlled trials have shown inconsistent effects on established cardiovascular risk markers such as inflammation, blood pressure or lipids,28 29 and some varieties appear to lack evidence of CVD benefit altogether.11 27 Indeed, tinned/canned fruit has been positively associated with all-cause and CVD mortality11 27 although the reasons for this observation are not clear and could potentially reflect socioeconomic status. One review only found cardioprotective effects for raw vegetables11; however, more varieties were associated with reduced all-cause mortality. It is unclear whether the lack of cardioprotection is true or due to a lack of high-quality research on specific fruits and vegetables (figure 1).

Fruits and vegetables
Eggs
Eggs are a rich source of dietary cholesterol, typically containing 150–230 mg/egg. With the exception of eggs, prawns and liver, most foods rich in cholesterol are also high in saturated fat and it is well established that dietary saturated fat influences levels of circulating low-density lipoprotein-cholesterol (LDL-C) to a much greater extent than dietary cholesterol in foods.30 However, the association of egg consumption (and dietary cholesterol) with CVD remains controversial and confusing for patients, particularly those with existing heart disease. The lack of good quality evidence to support the restriction of eggs has resulted in a recent changes to guidelines with many removing any reference to limiting egg and cholesterol intake,1 3 although this is still highlighted in the most recent American guidelines from primary prevention of CVD.2
In a very recent analysis of prospective cohort data, Zhong et al 31 indicated higher consumption of eggs and dietary cholesterol was positively associated with incident CVD and all-cause mortality. These findings are inconsistent with those from previous prospective cohort studies32–35 and a large review of meta-analyses11 or other prospective studies26 showing no association or a benefit to egg consumption However, in Zhong et al, 31 the effects of egg consumption were modest, and based on self-reported dietary intake at baseline (with an average follow-up of 17 years) in a US population that may not be representative of a UK diet.
In a prospective cohort study of 0.5 million Chinese adults,32 a moderate level of egg consumption (up to <1 egg per day) was significantly associated with lower risk of CVD. This study demonstrated that each one-egg increment per week was associated with an 8% lower risk of haemorrhagic stroke. In a subgroup analysis of diabetic populations, greater egg intake was associated with increased rick of CVD and CHD.34 35 The relationship between egg intake and diabetes incidence is not specifically covered here, but the role of egg intake and CVD incidence in people with diabetes requires further consideration made for the overall dietary pattern. However, eggs are a low in calories, high in protein and contain numerous micronutrients. Given their nutrient profile, eggs can form part of a healthy cardioprotective diet (figure 2).

Eggs.
Dairy
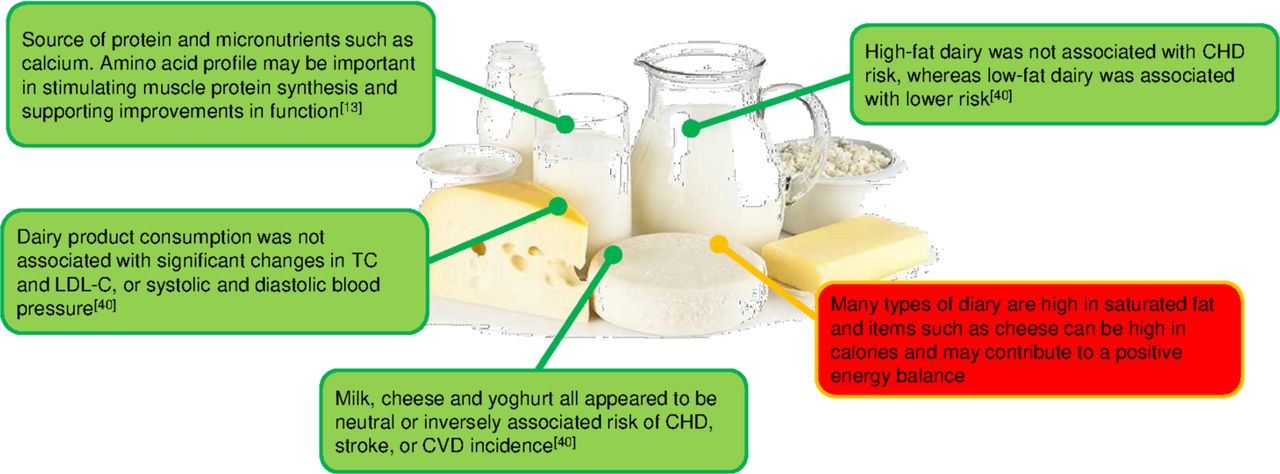
Dairy products have received a great deal of attention in terms of their effect on CVD risk primarily due to their saturated fat content of butter, whole milk and yoghurt, and most cheeses. However, there is increasing evidence that suggests dairy products may actually have a neutral or even a beneficial impact on CVD risk, and that some of the uncertainty in evidence may be related to the different types of dairy. This has been shown by Patterson et al 36 who also highlighted the importance of considering the calcium content of the food. In their analysis, the inverse association between total dairy intake and risk of MI was attenuated by adjustment for calcium with similar observations for cheese and MI risk.
Several recent systematic review and meta-analyses have continued to reinforce the inverse or neutral association between dairy intake and CV health.37–40 In a thorough review of systematic reviews and meta-analyses, Fontecha et al 40 confirmed no association between total dairy intake and CVD. When considering specific subtypes of CVD and dairy, high-fat dairy was not associated with CHD risk, whereas low-fat dairy was associated with lower risk. Milk, cheese and yoghurt all appeared to be neutral or inversely associated risk of CHD, stroke or CVD incidence. This paper also considered biomarkers in addition to the hard endpoints of CHD and stroke. Dairy product consumption was not associated with changes in TC or LDL-C. Similar results were also observed for systolic and diastolic blood pressure.
The effects of dairy intake appear to be relatively modest and in some studies, adjusting for total energy intake and consumption of other food groups (such as fruit, vegetables or red meat) can attenuate previously significant associations. Certain dairy products such as cheese are energy dense which could contribute to weight gain if consumed in excess. However, these same foods are high in amino acids known to stimulate muscle growth (leucine) and rich in calcium and phosphorus (figure 3).

Dairy.
Alcohol
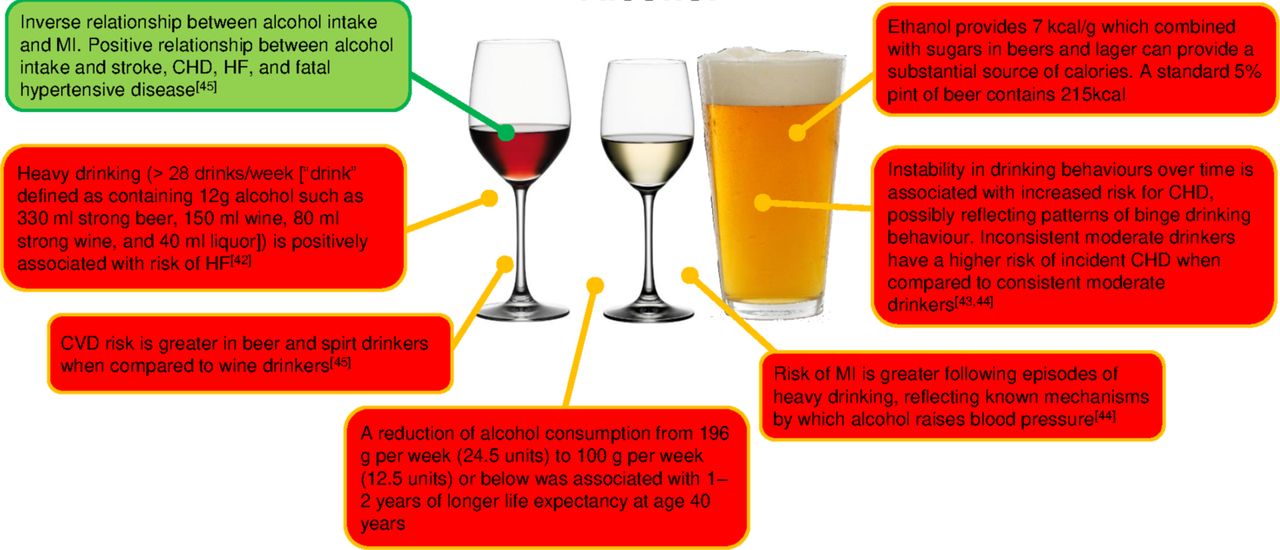
The relationship between alcohol consumption and CVD is still a subject of controversial debate in both primary and secondary prevention. Several meta-analysis have indicated inconsistent relationships between alcohol intake and cardiovascular health.41–45 A recent meta-analysis41 of 45 studies has shown a significant reduction of CHD mortality for low-volume drinkers and current drinkers comparing to abstainers. In all studies combined, low-volume alcohol consumption was associated with a significantly lower risk of CHD mortality. However, in those studies that excluded participants with heart conditions, low-volume consumption was not associated with reduced CHD mortality.41
Drinking patterns are also important to consider in the context of alcohol intake, and compared with moderate drinkers, those individuals who consumed a moderate volume of alcohol but did so more inconsistently had a higher risk of CHD mortality.43 This pattern of drinking may partly explain increased risk of an acute MI following a period of higher drinking44 and indicates that alcohol use does not have a uniformly protective effect against MI. Patterns of high consumption (perhaps reflecting the social context of alcohol consumption such as binge drinking) must be considered.
A criticism of studies in this area is a lack of acknowledgement that alcohol may have a differential effect on specific types of CVD. Consuming >100 g ethanol/week had a higher risk of all-cause mortality although a J-shaped relationship existed for all CVD outcomes.45 When this was disaggregated, alcohol intake (per 100 g/week higher consumption) was positively associated with stroke, CHD, HF and fatal hypertensive disease. With MI as the outcome, there was an inverse log-linear association with alcohol intake. These findings demonstrate how the consistency in frequency and low quantity of alcohol may play an essential role in cardioprotection and prevention. More evidence in needed in those individuals with a previous history of MI (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Alcohol.
Whole diet approaches
Studies considering whole diet approaches for CVD prevention are shown in online supplementary table 3.
The previous discussions have highlighted the complexities of nutrition. It is the view of the BACPR diet working group that nutrition research—especially that which impact directly on patients—be focused on food.
Improving diet quality post-MI is associated with a reduction in risk for all-cause mortality, with evidence to suggest it is the whole diet—rather than individual components—that drives this association.46 The most widely studied diet pattern in relation to cardiovascular health is the ‘Mediterranean’ diet (MedDiet), with multiple studies suggesting this diet pattern is associated with lower all-cause mortality in both primary and secondary prevention of CVD.47 48 Broadly speaking, this diet pattern contains a high nutrient density, is rich in fibre, has a relatively high intake of fat (predominantly from olive oil), low intake of saturated fat and a relatively low glycaemic index in comparison to Western diets. Traditionally, it is based around vegetables and fruits, nuts, legumes, and unrefined cereals, moderate fish and shellfish, and fermented dairy products in moderate amounts48 but will clearly differ pending on geographical region (eg, Spain vs North Africa). Greater adherence to an ‘Alternate MedDiet’ characterised by a high intake of vegetables, legumes, fruit, nuts, whole-grain cereals, fish, a high intake of monounsaturated fats, and low consumption of saturated fat, red and processed meats was associated with a pooled relative risk for all-cause mortality of 0.81 in post-MI individuals.47 In this same study, a two-point increase in the alternate MedDiet score was associated with a 7% decrease in all-cause mortality post-MI. This observed level of risk-reduction is also consistent across many other cohort studies examining the association between MedDiet adherence and all-cause and CV mortality.48 The authors of this study make a clear point that pizza consumed in non-Mediterranean countries should be considered as a type of fast food as it is high in calories, sodium and saturated fat due to the manufacturing process. Similarly, using canola oil (high in polyunsaturated fat) is technically not part of the traditional MedDiet. This means healthcare professionals should be prepared to correct preconceived ideas regarding what is and is not, a MedDiet. Aside from oil type, authorities agree large component of the cardioprotective diet is fruit and vegetables. The established DASH diet (rich in fruits and vegetables, whole grains, low-fat dairy, nuts, legumes, and low in red and processed meat) is associated with decreased incidence of stroke, CVD, CHD, diabetes, in addition to improvements in biomarkers such as systolic and diastolic blood pressure, haemoglobin A1c (HbA1C) and fasting insulin.49 The most recent analysis of this topic showed a benefit for greater incorporation of healthy plant foods into the diet, although this benefit was not seen with unhealthy sources (such as refined cereals). Compared with the lowest quintile, those individuals in the highest quintile of a plant-based diet had a lower risk of incident CVD, CVD mortality and all-cause mortality.50 Significant reductions in CVD and mortality endpoints were not observed with an unhealthy plant-based diet. Comparing these studies, it can be determined that not all plant-based diets are created equal. More research is needed into plant-based diets and their direct effects post-MI.
A growing area of interest is low-carbohydrate diets and a criticism of the studies cited so far is a lack of consideration of patient subgroups (ie, those with MI vs those with MI +type 2 diabetes mellitus). In this latter group, more aggressive control of carbohydrate intake may be justified and lead to better clinical outcomes. There is a lack of robust clinical evidence for low-carbohydrate diets post-MI and more research is needed in this field. In one recent study, a very low-carbohydrate diet was effective at improving diabetes-related outcomes (HbA1c and diabetes-related drug use) in addition to reducing triglycerides and increasing high-density lipoprotein cholesterol.51 The group did exhibit increases in TC and LDL-C which could be argued to be a negative consequence of the diet intervention, especially if extrapolated to a post-MI population. However, this same group showed previously that this increase in LDL-C was accompanied by a decrease in LDL particle number and an increase in LDL particle size52 (suggestive of a more favourable lipid profile). However, it is worth highlighting that there is substantial variation in response to low-carbohydrate diets so monitoring of lipids is important. This study was criticised at the time for patients self-selecting their intervention (not randomised to either treatment or control arm) although this in many ways represents a ‘real-world’ approach whereby patients are given a choice in their treatment. It is crucial to examine the carbohydrate replacement element and its source (fat vs protein, and animal or plant sources) as this will also govern the impact this diet pattern has on CV health. Indeed, a recent meta-analysis has indicated a plant-based low-carbohydrate diet is inversely associated with lower risk of mortality whereas an animal-based low-carbohydrate diet was positively associated with the same outcome.15 This highlights the importance for healthcare practitioners to explore diet choices with their patients, and not automatically assume plant-based or low-carbohydrate diets are ‘good’ and ‘bad’, respectively.
Conclusion
Recommendations from the working group are summarised in table 4. Focusing on macronutrients can be problematic with advice such as ‘reduce saturated fat’ and increase monounsaturated and polyunsaturated fats being vague and non-specific. The greatest improvement in cardiovascular outcomes will be seen when patients are provided with food-based advice. This requires those dispensing this information to have an understanding of nutritional science and an appreciation for the patients’ comorbidities. While there is a large body of evidence for the role of the MedDiet, additional approaches should be used in the right groups of patients. Low-carbohydrate diets can be carefully planned and be very nutritious, although similar to plant-based diets they can also be poor quality if not planned appropriately. Nutritional advice needs to be patient-focused, flexible, and should be adapted to each individual with CVD and their other comorbidities. More specialised dietitians are required in this area to guide the multi-professional team and provide guidance and training to those involved in the individual’s rehabilitation journey.
Summary recommendations
Acknowledgments
The authors acknowledge their colleagues for their comments and feedback on the manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @drtom_butler, @@conorkerley
Contributors All authors contributed equally to the searches, design and writing of the manuscript.
Funding This publication was supported by the British Association for Cardiovascular Prevention and Rehabilitation (BACPR)
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.