Article Text

Statistics from Altmetric.com
Transvenous lead extraction (TLE) has undergone an explosive evolution since its inception as a rudimentary skill with limited technology and therapeutic options. Early techniques involved simple manual traction that frequently proved ineffective for chronically implanted leads and carried a significant risk of myocardial avulsion, tamponade, and death.1 2 The significant morbidity and mortality associated with these early extraction techniques limited their application to life threatening situations such as infection and sepsis. The past 30 years have witnessed significant advances in lead extraction technology resulting in safer and more efficacious techniques and tools, providing the skilled extractor with a well equipped armamentarium. With the development of the discipline, we have witnessed a growth in the community of TLE experts coincident with a pronounced decline in the incidence of procedure related morbidity and mortality, with more recent registries at high volume centres reporting high success rates with exceedingly low complication rates (figure 1).3–6 Future developments in lead extraction are likely to focus on new tools that will allow us to provide comprehensive device management, alternative systems for extraction training, and the design of new leads conceived to facilitate future extraction.

Success, morbidity and mortality in large series. Graphic representation of complete success as a function of time, represented by black columns. Secondary y axis represents percentage morbidity (orange) and mortality (red). Timeline of extraction techniques and tools commensurate with reported trials is at the top of the figure. Values below the graph represent the number of leads (N) extracted in each study. Composite major complication (MC) and mortality (M) rate was calculated. Only studies with ≥50 leads extracted and data regarding mortality and major complications were included.
Pathology of the human–lead interaction
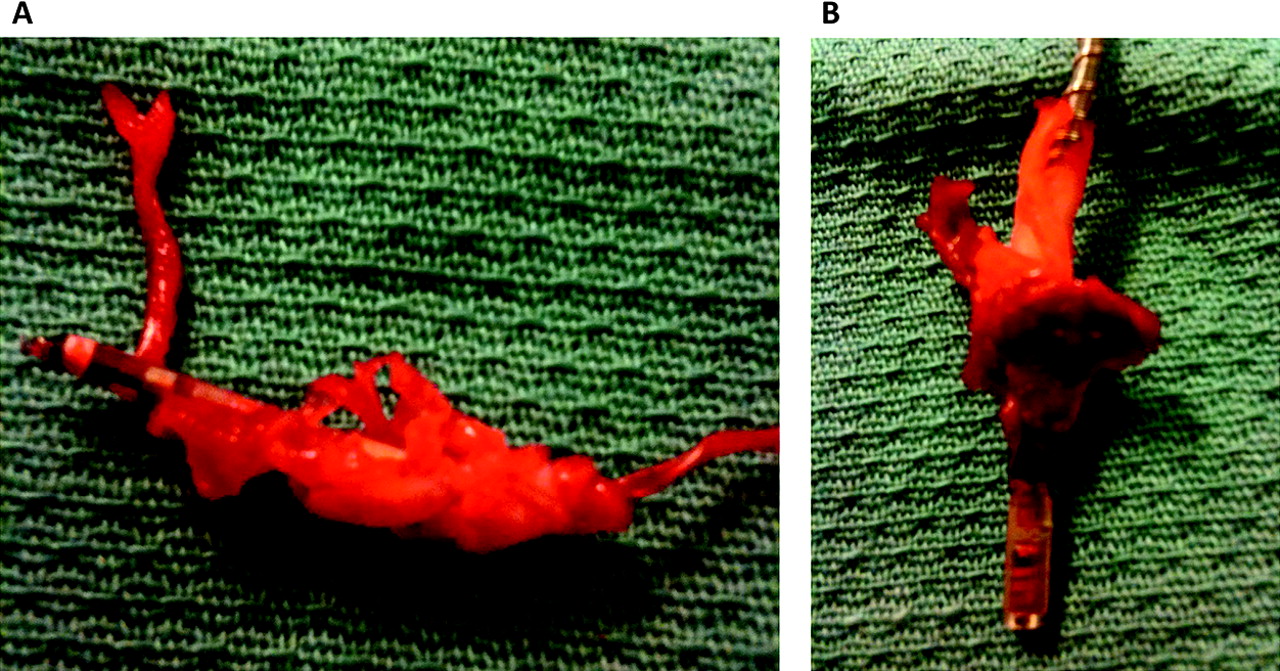
The challenges and risks of TLE are principally related to the body's foreign body response to a cardiovascular implantable electronic device (CIED). This response begins at implantation with thrombus development along the lead. Fibrosis of the thrombus occurs next with near complete encapsulation of the leads with a fibrin sheath within 4–5 days of implant.7 8 Robust fibrosis develops in areas of direct contact between the lead and the vasculature and endocardium (figure 2). The most common adhesion sites include the venous entry site, the superior vena cava (SVC), and the electrode–myocardial interface, and multiple areas of scar tissue are found in the majority of patients.9 Calcification of the fibrotic lesions can occur with time, further cementing the adhesion site and increasing the difficulties and risks of the extraction. Although predictors of severe scar formation have not been clearly identified, it appears that younger patients develop more vigorous fibrotic responses and more frequently develop progressive calcification.10 In addition to human–lead interaction, lead–lead binding can result in a significant challenge to extraction. Thus, multiple leads and duration of implantation are factors impacting the safety and efficacy of extraction. This is one of the arguments against abandoning superfluous leads.

(A, B) Fibrosis in areas of direct contact. Vigorous fibrosis develops in areas of direct contact between the lead and the vasculature and myocardium. (A) Extracted atrial lead with intense fibrosis at its distal portion. (B) Extracted defibrillator lead found to have a large amount of organised fibrosis at the electrode tip–myocardial interface.
TLE indications
TLE indications have expanded to include more clinical situations as advances in extraction techniques have made the procedure safer and more successful.11 The recently published 2009 Heart Rhythm Society (HRS) Expert Consensus Statement on TLE has extended class I indications to include patients with CIED pocket infection, occult gram-positive infection, and functional leads that, due to design or failure, may pose an immediate threat if left in place (table 1). The class II indications for TLE were further divided into IIa (reasonable to perform the procedure) and IIb (may consider performing the procedure) indications. CIED patients with occult gram-negative bacteraemia, severe chronic pain, ipsilateral venous occlusion with contraindication to contralateral implantation, non-functional leads, and need for MRI with no other imaging alternatives, and in whom implantation would result in more than four leads on one side or more than five leads through the SVC, represent class IIa indications for TLE. Class IIb indications for TLE include CIED patients with superfluous functional or non-functional leads and with functional leads that pose risk of device interference or that, due to design or failure, pose potential future risk.
Indications for transvenous lead extraction11
In assessing an individual's indication for TLE, a comparison of the risks of extraction with the risks of lead abandonment is mandated (figure 3). The consideration of patient and lead characteristics and, importantly, operator experience must be factored into the risk assessment of extraction. The risk assessment evaluation must include specific attention to the number of leads, implant duration, defibrillator versus pacing electrodes, and patient age.
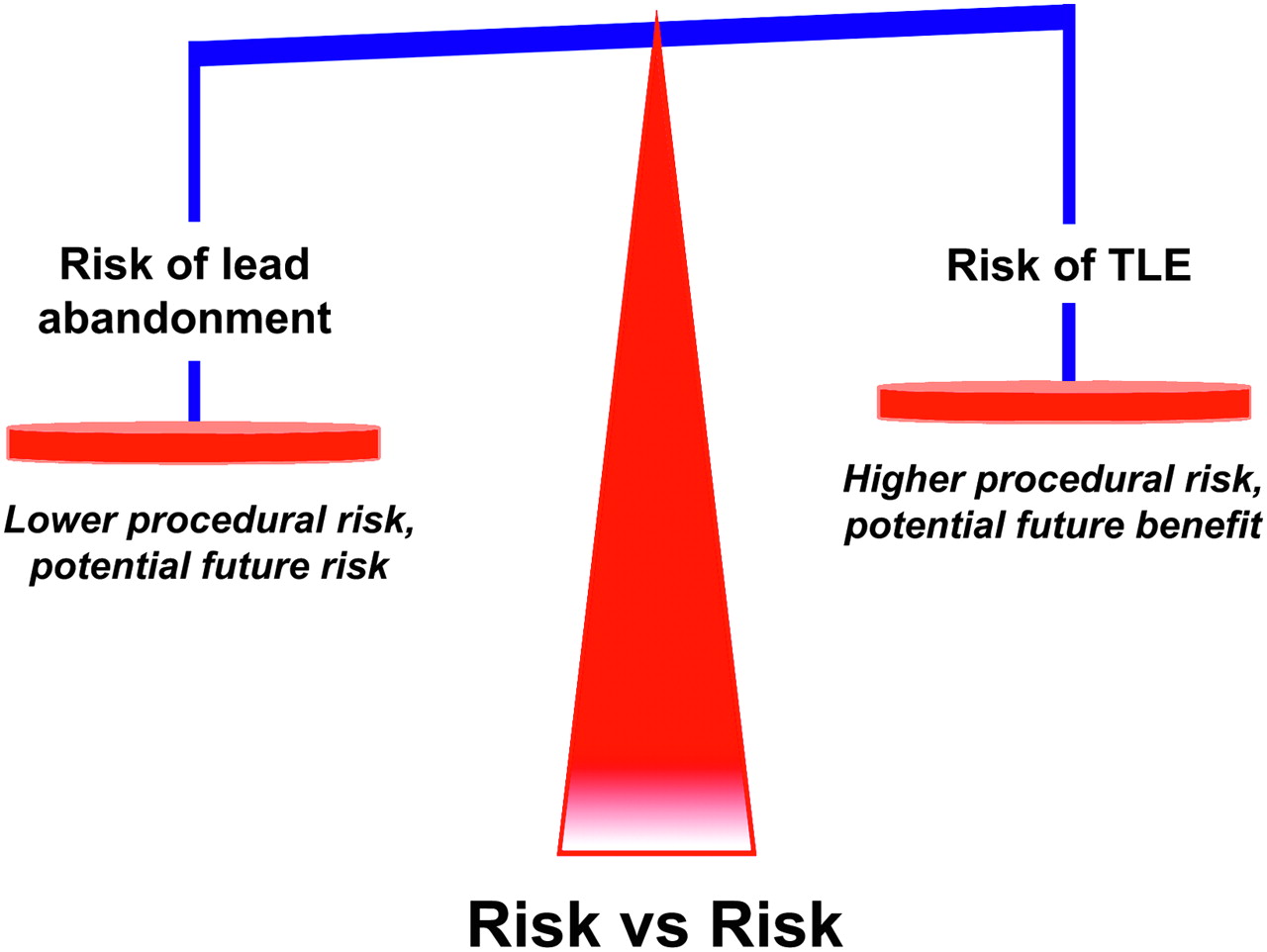
Risk versus risk. The decision regarding lead extraction or abandonment requires comparison of the current risks of lead extraction with the future risks of both lead abandonment and potential lead extraction. TLE, transvenous lead extraction.
Decisions regarding lead extraction must be made on an individual case-by-case basis integrating various patient and lead characteristics and operator related variables. Lead extraction with the potential for significant morbidity and mortality may not be warranted in patients with a poor prognosis or where the risks of intervention clearly outweigh the risks of lead abandonment. Additionally, those inexperienced in the procedure should not perform lead extractions, and nor should those without the necessary tools available to attain complete success or in a setting not prepared and committed to the complete and safe performance of the procedure.11
TLE techniques and tools
Pre-procedure and patient preparation
TLE, like any surgical procedure, requires a team approach with anticipation of and planning for all potential situations. The required personnel of the extraction team include, at a minimum, the physician performing the extraction, a cardiothoracic surgeon, anaesthesia support, an x ray technician or other person to operate the fluoroscopy, and both scrubbed and non-scrubbed assistants. While complications will occur, the single most important factor in preventing a major complication from resulting in a death is the time to intervention. Thus, the procedure location—that is, the operating room or catheterisation or electrophysiology laboratory—is less important than the immediate availability of cardiothoracic surgical intervention. This mandates that a surgeon proficient at managing the potential complications be on site during the extraction procedure and that the equipment necessary for cardiopulmonary bypass be readily available. Additional emergency equipment that should be present in the room or immediately available includes transthoracic and/or transoesophageal echocardiography, a pericardiocentesis tray, vacuum containers for chest tube drainage, temporary pacing equipment, an anaesthesia cart for general anaesthesia, and vasopressors and other emergency medications. We have fashioned a mobile ‘extraction cart’ that contains all the aforementioned emergency equipment in addition to extraction tools (locking stylets, non-powered and powered sheaths, femoral workstations, extraction snares, etc) and CIED implant tools (stylets, wrenches, fixation tools, introducer sheaths, intravenous contrast, repair kits, etc).
Recognising the potential need for emergent surgical intervention (table 2), our patients are prepared for the procedure in such a way so as to eliminate any delays. We prep our patients with a chlorhexadine solution and drape so as to allow access for contralateral implant or emergent pericardiocentesis, thoracentesis, thoracotomy, sternotomy or cardiopulmonary bypass. It is our practice that all patients have bilateral peripheral venous access with large bore catheters, femoral venous access, invasive haemodynamic monitoring with a radial arterial line, general endotracheal anaesthesia, and four units of packed red blood cells immediately available.
Potential complications of transvenous lead extraction
Techniques
We employ a stepwise approach to lead extraction in every case with the goal of complete success utilising the least amount of tools (figure 4). As we routinely perform TLE by the superior approach via the implant vein, the initial step in the extraction procedure is an appropriately positioned incision that permits easy access to the venous entry site in a plane parallel to the leads. It is our practice to attempt to use the existing incision whenever possible and perform an elliptical incision excising the existing incisional scar. Occasionally, two incisions are necessary—one over the venous entry site of the leads and a second over the pocket or area of skin erosion or adherence. Once the pocket is entered, microbial cultures of pocket tissue are obtained in all cases of CIED infection. Then, the device is removed and the leads are dissected free back to their venous entry site. Dissection around the venous entry site is important to allow easy passage of any devices that may be necessary for lead extraction, but aggressive dissection can result in transient issues with haemostasis secondary to back bleeding. The anchor sleeves are then removed and all extraneous material, including suture material, is eliminated from the pocket. Complete removal of infected tissue and foreign material is mandatory in cases of CIED infection. Additionally, it is our routine practice to perform a capsulectomy whenever ipsilateral reimplantation is planned.

Stepwise approach to lead extraction. We routinely employ a stepwise approach to lead extraction so as to achieve the highest rate of complete success utilising the least amount of tools. CTS: countertraction sheath, including mechanical dilating sheaths, laser sheaths or mechanical cutting sheaths.
If ipsilateral reimplantation is planned, ipsilateral venous access is attempted under fluoroscopic guidance with or without the aid of intravenous contrast. In our experience, stenotic lesions can often be crossed with use of a 5 French dilator and glidewire. If the vein is successfully cannulated and a wire could be passed into the inferior vena cava, or if ipsilateral reimplantation is not planned, lead removal with simple traction is attempted. If this proves unsuccessful, the lead is cut and a locking stylet is introduced, a number 5 silk is tied around the lead body, and traction reattempted. The number 5 silk is used to reinforce the lead and to prevent the insulation from bunching up or ‘snow plowing’ under the force of counterpressure. If lead removal still proves unsuccessful, a non-powered or powered sheath is employed. Sheath selection is determined by the clinical situation and the operator's preference and experience. If the lead is not retrievable from the implant vein or lead disruption occurs, transfemoral retrieval is performed.
Counterpressure, traction, and countertraction
Counterpressure is the force applied by the non-powered or powered sheath as it is advanced over the lead interrupting areas of adherent scar tissue. Sufficient traction must be applied to the lead and locking stylet so the lead acts as a ‘rail’. This allows the sheath to follow the lead body and not damage the vasculature as the lead curves within the vein. This is especially true when passing the sheath from the brachiocephalic vein through the SVC to the right atrium. By exerting significantly more ‘pull’ than ‘push’, lateral force on the SVC can be reduced. Countertraction is a technique employed once the sheath has been advanced to the lead tip–myocardium interface. Applying countertraction limits the traction forces on an entrapped electrode to the circumference of the sheath at the lead tip–myocardium interface. Once the lead is released from the fibrous tissue, the myocardium falls away from the sheath, reducing the risk of myocardial invagination and injury (figure 5).12–14

Counterpressure, traction, and countertraction. Schematic representation of the forces of counterpressure, traction, and countertraction. Counterpressure is the force applied by the non-powered or powered sheath as it is advanced forward over the lead interrupting areas of adherent scar tissue. Traction is the pulling force on the lead to provide a straight ‘rail’ so as to allow the sheath to follow the lead. Countertraction is the forward force applied by the sheath at the myocardium to limit the traction forces on an entrapped electrode to the circumference of the sheath at the lead tip–myocardium interface. Once the lead is released from the fibrous tissue, the myocardium falls away from the sheath, reducing the risk of myocardial invagination and injury.
Approaches
Leads are typically extracted by a superior approach via the implant vein, although alternative approaches are used in certain situations. For example, when the free lead tip cannot be reached from the implant vein, an inferior approach via the femoral vein is necessary. Occasionally, hybrid or alternative venous approaches are utilised. The success of a combined approach via the femoral and internal jugular veins for free-floating leads and leads with dense SVC adhesions has been reported by Bongiorni and colleagues.5 Lead stabilisation by femoral snaring via an inferior approach provides a straighter ‘rail’ for the extraction approach from the right internal jugular vein, decreasing the likelihood of SVC avulsion. Recently, Fischer et al15 described a hybrid superior and inferior approach, with femoral snaring of the lead to provide stability from below while counterpressure and traction were applied from above. They demonstrated this to be a safe and effective technique for lead extraction with maintenance of venous access.
Tools
Locking stylets
The ability to extract a lead with traction successfully is directly dependent upon the lead construction and its tensile strength.10 Locking stylets were developed to reinforce the lead, transmit the extraction force to the tip of the lead, reduce the risk of lead disruption, and increase the likelihood of complete lead removal.12 16 17 Several types of locking stylets have been designed. While the original locking stylets had to be sized to the luminal diameter of the conductor coil, the most commonly utilised locking stylets today are designed to accommodate a range of conductor coil diameters. The Liberator (Cook Medical, Bloomington, Indiana, USA) and Lead Locking Device (LLD) EZ (Spectranetics, Colorado Springs, Colorado, USA) stylets offer similar support but differ in their locking mechanism design. The locking mechanism of the Liberator is at the distal tip of the stylet providing focal traction at the tip of the lead, whereas the LLD EZ stylet grabs the lead in multiple areas and exerts force along the length of the lead (figure 6A,B). If a lead cannot receive a locking stylet, either due to extensive damage or a solid core design, applying sufficient traction can prove challenging. The Bulldog Lead Extender (Cook Medical) is a tool that can be useful in this situation (figure 7). It consists of a wire with a threadable handle through which the lead is passed and secured, thereby locking the insulation and conductor to the extender. The advent of locking stylets has permitted safer and more successful TLE via the implant vein, stimulating the development of new techniques and technologies.

(A, B) Locking stylets. (A) The Liberator Locking Stylet (Cook Medical, Bloomington, Indiana, USA) fits leads with lumen diameters of 0.016–0.032 inches. An undeployed Liberator locking stylet is shown above a deployed Liberator locking stylet. When deployed, the wound spring at the end of the stylet opens up, locking into place. (B) The Lead Locking Device (LLD) EZ (Spectranetics, Colorado Springs, Colorado, USA) has a radiopaque tip and accommodates inner coil diameters of 0.015–0.026 inches (undeployed stylet, top image). In contrast to the Liberator locking stylet, the LLD locking stylet has a braided mesh over the entire length of a solid lead that expands when deployed (bottom image).

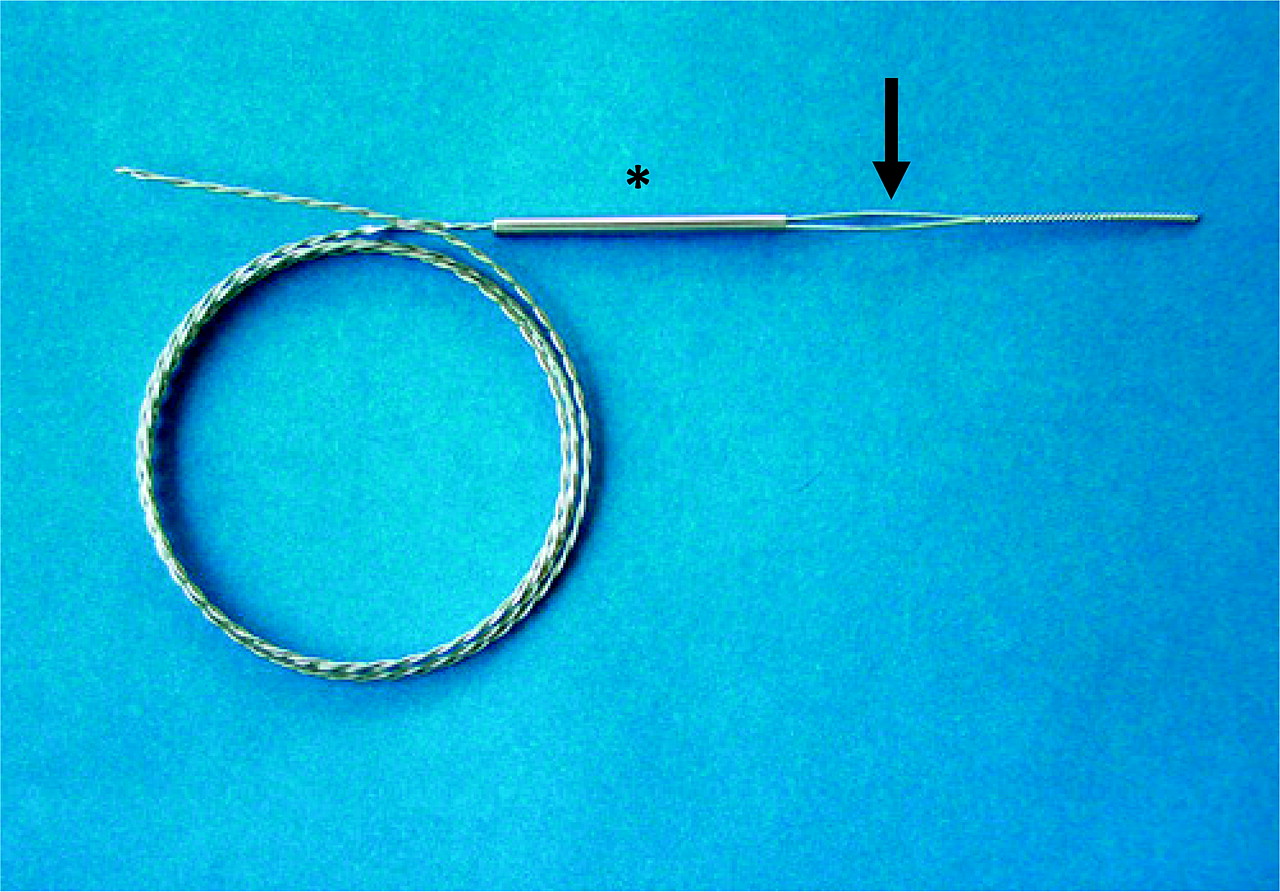
Bulldog Lead Extender (Cook Medical, Bloomington, Indiana, USA). The Bulldog Lead Extender is a useful tool for leads that cannot receive a locking stylet, either due to extensive damage or a solid core design. The exposed end of the lead is passed through the loop of the Bulldog (arrow) and the metal sleeve (asterisk) is advanced over the loop grasping the lead.
Telescoping sheaths
Telescoping sheaths are non-powered sheaths available in a range of sizes from 7–16 French and made of different materials with varying properties, including stainless steel, Teflon, and polypropylene (figure 8). Teflon is soft and flexible but is unable to cut through dense scar tissue, while polypropylene is stiffer and better at disrupting encapsulating scar but must be used with caution so as to avoid vascular injury. Stainless steel sheaths are employed only for disrupting dense and calcified fibrosis as the central venous circulation is entered. The inner and outer sheath pair is advanced along the lead with alternating counterclockwise and clockwise motions with moderate pressure. The soft inner sheath is used as a guide while the more rigid outer sheath serves to disrupt and dilate the encapsulating fibrous tissue. Sufficient traction is essential to ensure that the sheaths track the path of the lead and remain within the confines of the vasculature under fluoroscopic guidance. Utilising telescoping sheaths, TLE success rates via a superior (ie, implant vein) approach range from 71–97%.12 14 16 18

Telescoping non-powered countertraction sheaths. Telescoping sheaths are available in a range of sizes from 7–16 French and made of different materials with varying properties, including stainless steel, Teflon, and polypropylene (from left to right).
Powered sheaths
Powered sheaths employ a source of energy to make the dissection of encapsulating fibrous tissue easier and more efficient, thus enabling the advancement of the sheath along the lead with reduced countertraction and counterpressure forces.10 19 One such powered sheath is the Excimer Laser System (Spectranetics), a ‘cool’ pulsed ultraviolet laser at a wavelength of 308 nm available in 12, 14 and 16 French sizes. The laser sheath applies circumferential pulses of energy at its distal end, dissolving tissue in contact with the tip of the sheath by photochemical destruction of molecular bonds and photothermal ablation that vaporises water and ruptures cells, with resultant photomechanical creation of kinetic energy (figure 9A,B).20 The sheath is advanced over the lead body utilising the standard techniques of counterpressure and countertraction, and laser energy is delivered when encapsulating fibrous tissue halts sheath advancement. Tissue in direct contact with the sheath tip is ablated to a depth of 50 μm until the distal electrode is reached; countertraction is still necessary to dislocate the lead tip. Compared with mechanical telescoping sheaths, laser assisted extraction resulted in more frequent complete lead removal and shortened extraction times without an increase in procedural risk.21–23 The introduction of laser extraction changed the landscape of transvenous extraction, providing a highly effective and low morbidity technique with broad applications.6 21 23

(A, B) Excimer laser sheaths (Spectranetics, Colorado Springs, Colorado, USA). (A) The Excimer laser sheath utilises ultraviolet laser energy to vaporise tissue in contact with the tip of the sheath where the optical fibres terminate. The sheath is available in a range of sizes (12 French, 14 French, and 16 French) displayed from top to bottom. (B) End-on view of the laser sheath demonstrating the distal end where the optical fibres terminate.
The Perfecta Electrosurgical Dissection Sheath (Cook Medical) represents another type of powered sheath. The electrosurgical dissection sheath consists of an inner polytetrafluoroethylene (PTFE) sheath with bipolar tungsten electrodes exposed at the distal tip and an outer sheath for counterpressure and countertraction. Radiofrequency energy is delivered between the bipoles to dissect through fibrous binding sites, much like a surgical cautery tool, although the lead tip must be liberated with countertraction. In contrast to the Excimer Laser Sheath, the Electrosurgical Dissection Sheath permits a localised application of radiofrequency energy with linear rather than circumferential dissection of the encapsulating fibrous tissue. The focused and steerable dissection plane offers the potential advantages of improved precision; however, the sheath may have to be repositioned repeatedly as a result. The Electrosurgical Dissection Sheath offers a cost effective alternative to the Excimer Laser System without compromising safety or efficacy.24
Despite the improved success rates of lead extraction with powered sheath technologies, disruption of calcified binding sites remains difficult with either system. The most recent addition to the armamentarium of lead extraction tools provides a solution. The Evolution and Evolution Shortie Mechanical Dilator Sheaths (Cook Medical) are ‘hand powered’ mechanical sheaths that consist of a flexible, braided stainless steel sheath with a stainless steel spiral cut dissection tip. The sheath is attached to a trigger activation handle that rotates the sheath and allows the threaded metal end to bore through calcified and dense adhesions (figure 10).25 In our experience, we have found the Evolution sheath quite useful for disrupting sites of calcified fibrosis, but often at the expense of functional leads that we were attempting to preserve. Regardless, this technology has provided an effective alternative for dealing with the challenges posed by densely scarred venous entry sites and heavily calcified adhesions.26
The Evolution device. The Evolution and Evolution Shortie Mechanical Dilator Sheath (Cook Medical, Bloomington, Indiana, USA) are ‘hand powered’ mechanical sheaths that consist of a flexible, braided stainless steel sheath with a stainless steel spiral cut dissection tip (inset). The sheath is attached to a trigger handle that rotates the sheath and allows the threaded metal end to agar out the scar tissue.
Femoral tools
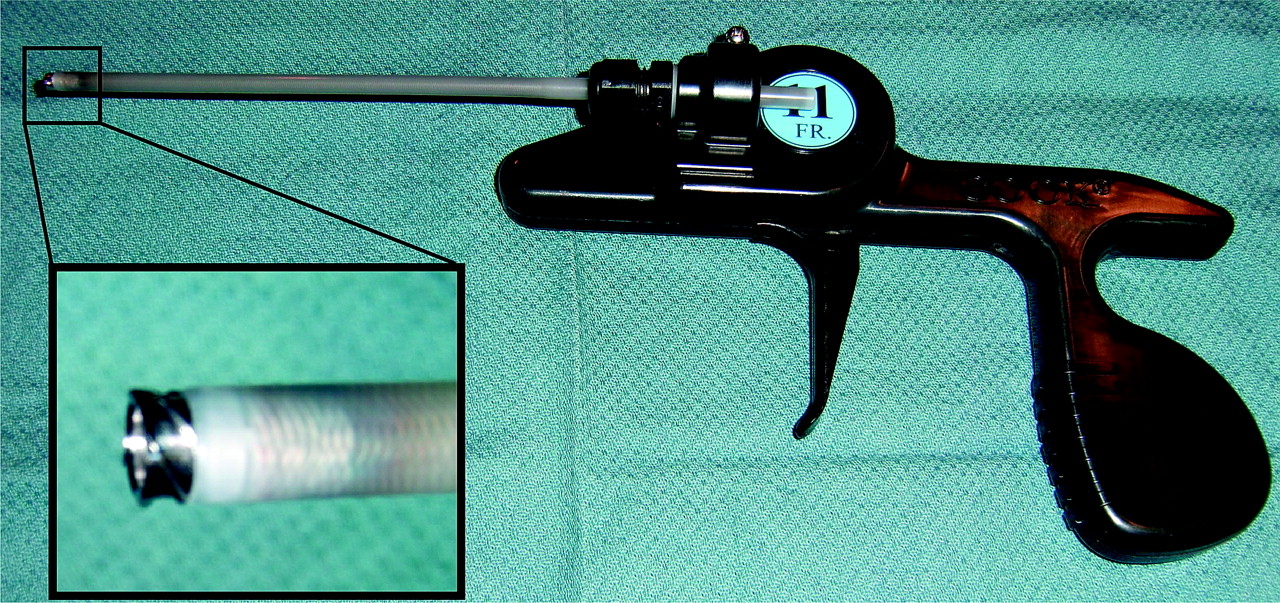
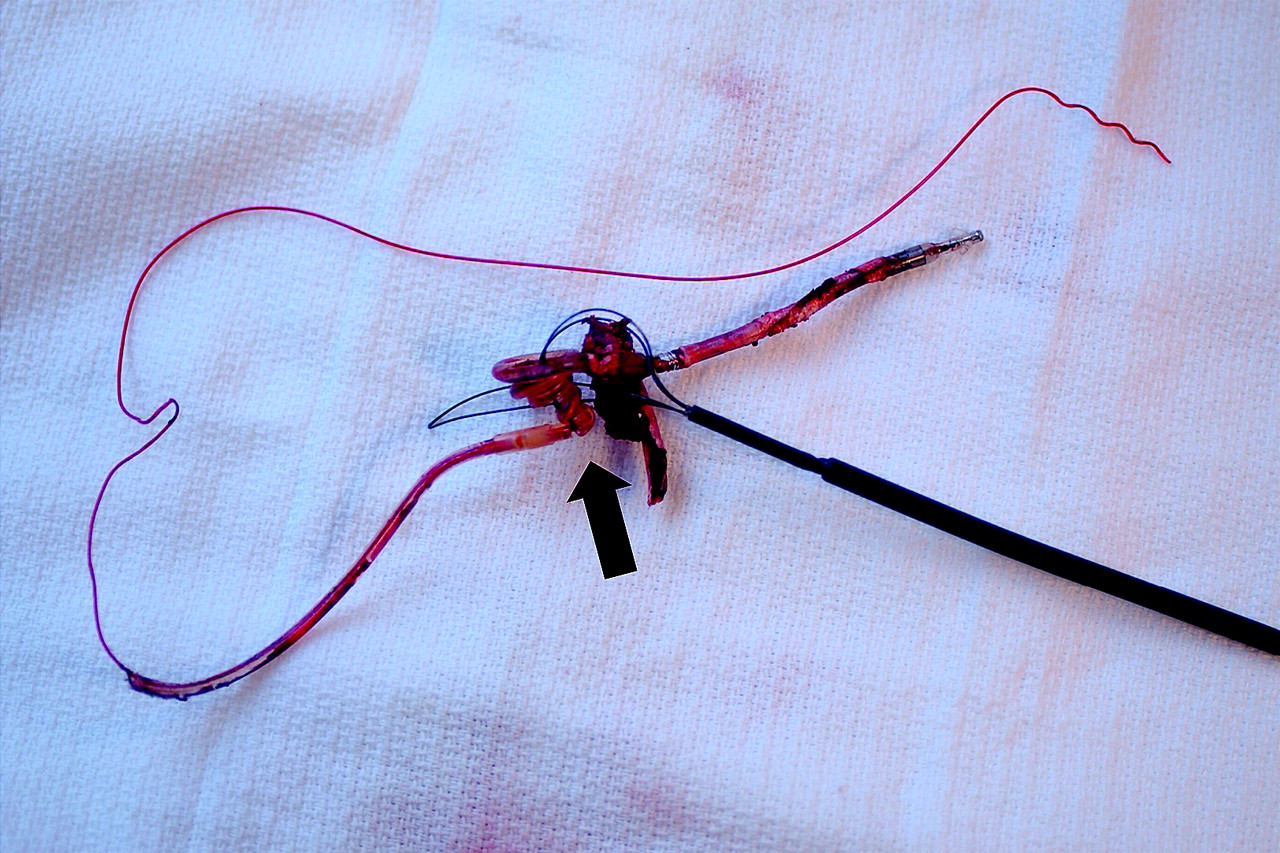
Transfemoral lead retrieval with the Byrd Workstation (Cook Medical) is a necessary skill for successful lead extraction, particularly in cases when the lead is not accessible from the implant vein as in a cut or fractured lead (figure 11). The Byrd Workstation consists of a 16 French outer sheath with a one-way valve that is advanced over a wire into the femoral vein, and a 12 French inner sheath through which a number of retrieval snares can be advanced. The Workstation package contains a Needle's Eye snare, but a number of other snares can be utilised including Tulip and Amplatz gooseneck snares. If lead retrieval with a Needle's Eye snare proves unsuccessful, we have found the combination of a gooseneck snare and bioptome forceps to be quite successful. We preload the gooseneck snare on the bioptome, advance the two together to the lead fragment, grasp the free lead tail with the bioptome, and then advance the gooseneck snare over the bioptome to ensnare the lead. The challenge of femoral retrieval remains manipulating the tools and snaring the lead in three dimensions using two dimensional fluoroscopic imaging. The recent description of a novel technology to facilitate extraction and the maintenance of vascular access proposed a hybrid superior and inferior approach, with femoral snaring of the lead to stabilise the lead while countertraction and counterpressure are used to free the lead, reiterating the clinical importance of femoral retrieval.15
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Transfemoral snaring of lead. Transfemoral lead retrieval with the Byrd Workstation (Cook Medical, Bloomington, Indiana, USA) is a necessary skill for successful lead extraction, particularly in cases when the lead is not accessible from the implant vein as in a cut or fractured lead. The lead has been snared and wound up by the Needle's Eye snare (arrow) allowing successful removal of the lead.
Outcomes
Early studies of TLE with a laser sheath such as the PLEXES trial demonstrated a pronounced improvement in extraction efficacy from 64% with traditional extraction techniques to 94% with laser assisted extraction without a significant difference in complications, although significant crossover between groups occurred.21 Coincident with the growth of the discipline of TLE, we have witnessed a notable decline in the incidence of procedure related morbidity and mortality, with a number of high volume single centres reporting morbidity and mortality rates less than 1.0% and 0.3%, respectively (figure 1).3–5 A recent multicentre study of transvenous laser lead extraction in 1449 patients demonstrated similarly low morbidity and mortality complication rates of 1.1% and 0.28%, respectively, with a higher clinical success rate of 98.8%. The operators in this study were from 13 centres and represented small (≤60 cases), medium (61–130 cases), and large volume (>130 cases) extraction centres, although the majority of sites consisted of medium and high volume extractionists with all extractors having significant experience.
Recently, Cook Medical initiated the LEADER database to gather ‘real world’ result data. The preliminary data demonstrate low major complication (1.2%) and mortality rates (0%) among predominantly low (≤2 extractions/month) and moderate (3–5 extractions/month) volume operators. These risks, in fact, are significantly less than other routinely performed cardiovascular procedures. For example, published major adverse events for atrial fibrillation ablation and percutaneous coronary intervention (PCI) procedures are several fold higher, with a reported 1–2% mortality rate with PCI.
Complication rates with TLE directly parallel operator experience. Major and minor complications are reduced by approximately 50% with increased operator experience from 20–120 cases to >300 cases performed.27 Large scale multicentre randomised trials have confirmed the effect of experience on outcomes.6 9 21 23 27 Likewise, observational registries of experienced, high volume extractionists have consistently demonstrated even higher success rates (>99%) with exceedingly low major complication (<1.0%) and mortality rates (<0.3%).3–5 Consequently, the 2009 HRS Expert Consensus Statement on Lead Extraction recommends that physicians being trained in TLE extract a minimum of 40 leads as the primary operator under the direct supervision of a qualified physician and extract a minimum of 20 leads annually to maintain their skills.11 This is a minimum recommendation; there are many who feel that the best outcomes come with additional experience. The ability for trainees and those post-training to gain this experience is limited. Recently, Spectranetics and others have begun the development of a realistic simulator to allow for those interested in performing extractions to practise, gain experience, and confront emergencies in a safe and controlled environment.
Future directions
TLE has evolved dramatically over the past 30 years and exponentially throughout the past decade. Despite these advances, the basic tenants of counterpressure, traction, and countertraction remain critical to ensuring successful and safe outcomes. As indications for device therapy expand and younger patients receive devices, it is likely that the number of lead extractions performed will increase, as will the pressure on the field to continue to evolve not simply as a technique but as a discipline and a science.
The 2009 HRS Expert Consensus on TLE provides several recommendations to help the specialty of lead extraction evolve. The document creates standard definitions, recommends guidelines for safe lead extraction, identifies indications for extraction, and emphasises the importance of reporting outcomes. As new extraction tools and novel leads designed to facilitate future extraction are introduced, standardised reporting of outcomes will become essential. Data collection will serve to advance our collective knowledge and allow us to draw conclusions regarding the safety and complications of these techniques. To date, questions regarding the benefits of lead extraction in specific situations remain and a nationwide database of extraction outcomes and complications will allow us to critically evaluate and rigorously answer these questions. Moreover, collaboration among those performing lead extraction will be critical to building a community of lead extractors and creating a field committed to quality. The future of lead extraction lies in the development of new techniques, tools and training methods, the creation of a collaborative community, and the growth of the science.
Challenges of transvenous lead extraction (TLE): key points
TLE has evolved dramatically since its beginnings in the 1980s.
The challenge and risk of TLE are directly related to the human–lead interaction.
Most common sites of scar formation include the venous entry site, superior vena cava, and electrode tip–myocardial interface.
Younger patients develop more robust scar formation.
TLE indications are outlined in the 2009 HRS Expert Consensus Statement on TLE.
Class I TLE indications have expanded to include pocket infections, occult gram-positive infection, and functional leads that may pose an immediate threat if left in place.
In assessing an individual's indication for TLE, the risks of extraction must be compared with the risks of lead abandonment.
TLE requires a team approach with anticipation of and planning for all potential situations.
Principles of counterpressure, traction, and countertraction should be applied to all TLE tools.
Several extraction tools are available and the extractionist should be well versed in all techniques as several different approaches can be necessary.
Several groups have reported major complication and mortality rates of less than 1% and 0.3%, respectively.
LExICon, a recent multicentre prospective observational study of laser lead extraction in 1449 patients, demonstrated a major complication and mortality rate of 1.1% and 0.28%, respectively.
Complication rates parallel operator experience.
Suggested minimum standards for training and maintenance of competency are 40 and 20 leads, respectively.
Standardised outcomes reporting is essential.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Recent, large prospective observational study of laser lead extraction including 1449 patients.
- ↵
- ↵
- ↵
- ↵
- ↵
Transvenous lead extraction consensus statement creating minimum educational standards, providing guidelines for the practice of transvenous lead extraction, and defining standardised outcome definitions.
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
First randomised controlled trial of laser lead extraction compared with mechanical dilating sheaths.
- ↵
Report of the US Lead Extraction Database, a large prospective observational registry.
- ↵
First prospective registry of large laser sheath (14 French, 16 French) experience.
- ↵
- ↵
- ↵
- ↵
A further report of the US Lead Extraction Database.
Footnotes
Competing interests In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article. Honorarium/Consultant for Spectranetics Inc.
Provenance and peer review Commissioned; internally peer reviewed.