Article Text

Abstract
Background Both mechanical thrombectomy and glycoprotein (GP) IIb/IIIa antagonists have been shown to improve clinical outcomes following primary PCI for ST segment elevation myocardial infarction. There is limited data describing the use of these technologies in the setting of stent thrombosis. We aimed to assess the combined approach of mechanical thrombectomy with adjunctive glycoprotein (GP) IIb/IIIa antagonists in patients presenting with acute stent thrombosis.
Methods This was an observational cohort study of 3040 patients who underwent PPCI from 2003 to 2011. The primary outcome was major adverse cardiac events (all cause mortality, myocardial infarction, target vessel revascularisation and stroke). Follow-up was for a median of 3.0 years (IQR 1.2–4.6 years). Patients were split into 3 groups; those who underwent PCI using mechanical thrombectomy and GP IIb/IIIa inhibitors, those receiving either GPIIb/IIIa inhibitor or mechanical thrombectomy and those receiving neither.
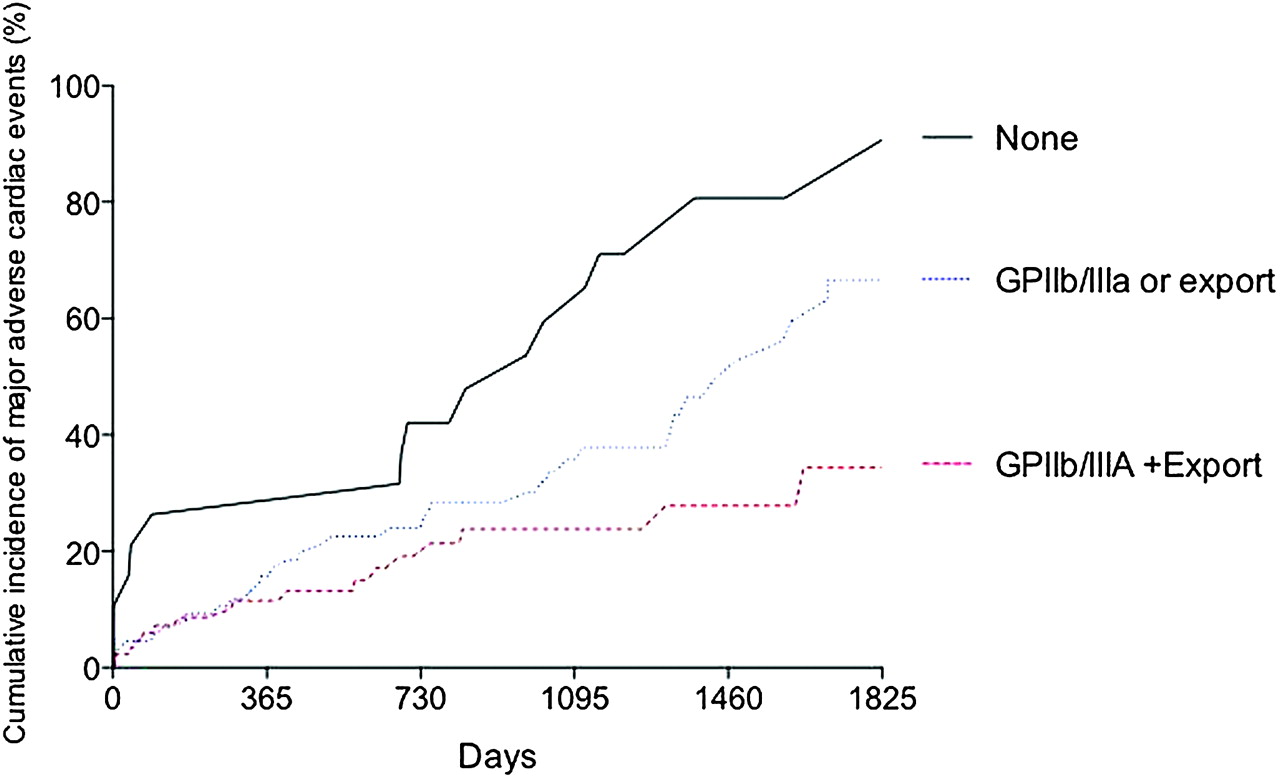
Results 201 patients (6.6%) of all STEMI patients presented with stent thrombosis (ST). Overall, GPIIb/IIIa inhibitors were used in 176 (87.6%) patients. Mechanical thrombectomy was used in 94 (46.7%) patients. 88 (44%) patients received both GPIIb/IIA inhibitors and thrombectomy, 92 (46%) received either GPIIb/IIIa inhibitor or thrombectomy and 21 (10%) received neither therapy. Baseline characteristics of these 3 groups are shown in Abstract 035 table 1. Patients receiving both therapies tended to have more successful procedures and have better post-procedural left ventricular function. Kaplan–Meier estimates of long-term major adverse cardiac events showed the lowest rates of events for those patients receiving both therapies, followed by those receiving a single therapy, with the highest rates of MACE in those receiving neither therapy (p<0.0001) (Abstract 035 figure 1). All individual component of MACE were lower in those receiving both therapies. Age-adjusted Cox analysis showed a decrease in the hazard of death for those receiving both therapies compared to those receiving neither (HR 0.17 (95% CIs 0.06 to 0.54) and this was maintained with multiple adjustment (HR 0.11 (95% CIs 0.02 to 0.85).
{kind=link}
Conclusion Prognosis after stent thrombosis is poor with high long-term event rates. Using a combined approach of mechanical thrombectomy with adjunctive GP IIb/IIIa blockade lead to effective primary PCI with improved long-term outcomes.
- Thrombectomy
- GP IIb/IIIa
- stent thrombosis