Article Text

Abstract
Background Anecdotal accounts suggest a differential approach to drug-eluting stents (DES) internationally and recent reductions in use following reports of late stent thrombosis. Current studies of clinical practice are limited in their scope. We aimed to analyse trends in DES utilisation in four international healthcare and regulatory settings.

Drug-eluting stent (DES) use by registry (smooth estimate with 95% CI).

{kind=link}
{kind=link}
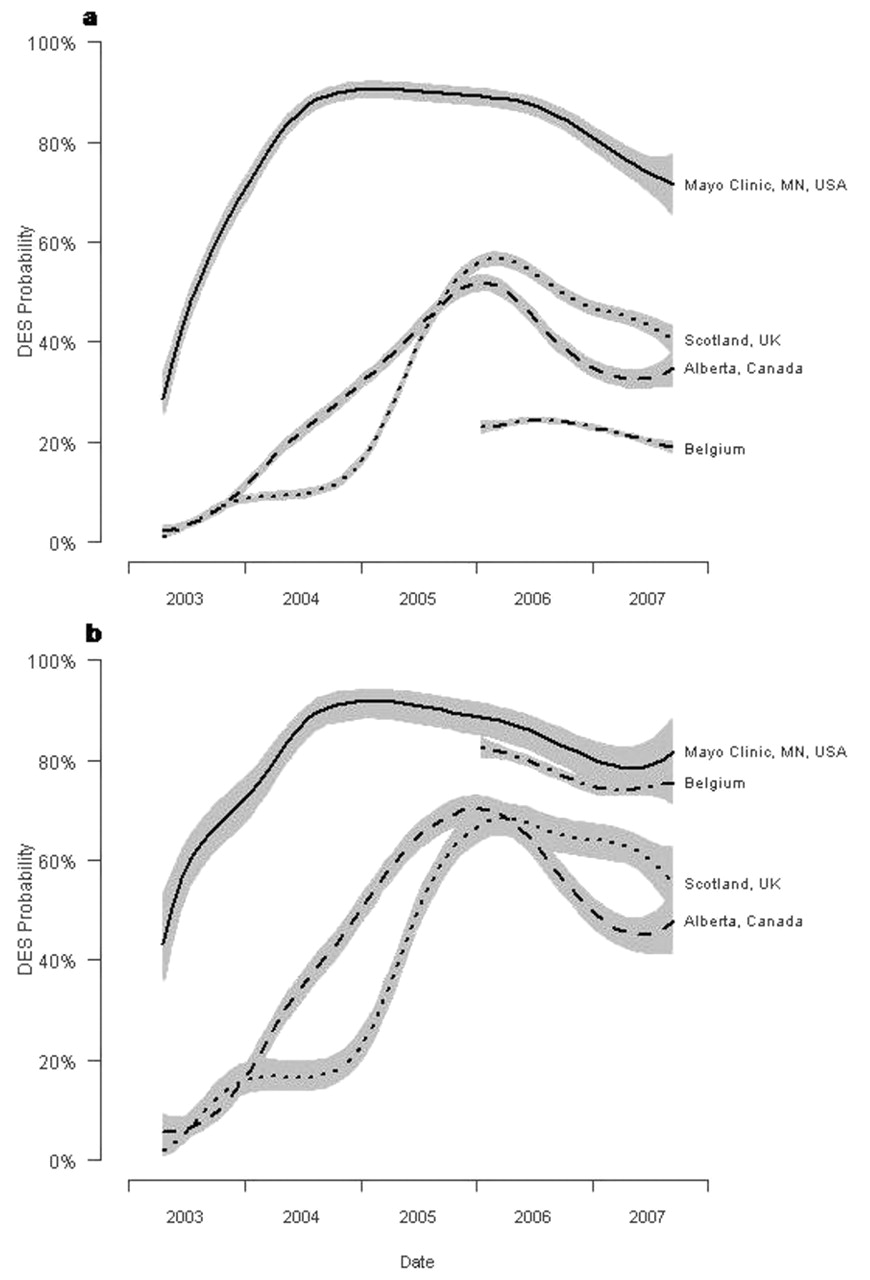
Drug-eluting stent (DES) use by registry for (a) patients without diabetes; (b) patients with diabetes (smooth estimate with 95% CI).
Methods Data were pooled from angioplasty registries in Alberta (Canada), Belgium, Mayo Clinic (Minnesota, USA) and Scotland (UK), which have routinely recorded consecutive patients treated since 2003 (table). Type of stent (DES or bare-metal stent) was determined and data were analysed at the level of the lesion. To allow the graphical presentation of time trends in DES use with 95% CI, local likelihood-based non-parametric logistic regression estimates by country were calculated. An overall model was constructed for DES use by country, then separate models were stratified by key clinical subgroups: lesion length (<16 mm, 16–30 mm, >30 mm), vessel diameter (<3 mm, ⩾3 mm), diabetic status and clinical indication (stable/unstable angina, non-ST elevation myocardial infarction, ST elevation myocardial infarction). Only the overall model and diabetic subgroups are presented due to space constraints.
Results 178 504 lesions treated between January 2003 and September 2007 were included in the overall analysis (fig 1). In the Mayo Clinic Registry there was rapid adoption to a peak of 91% DES use by the end of 2004, with little variation by clinical subgroup. In contrast, Alberta and Scotland showed delayed adoption, with lower peak DES use, respectively, 56% and 58% of lesions by early 2006. Selection of patients at high baseline risk of restenosis, such as long lesions, small vessels and those with diabetes (fig 2), was evident throughout. Adoption of DES in Belgium was more gradual and peak use of 35% lower than other registries (fig 1). The use of DES in Belgium strongly favoured patients with diabetes (fig 2). Variable reductions from peak use were seen in all datasets during 2006: Mayo Clinic 16% absolute/18% relative reduction, Scotland 16%/28%, Alberta 19%/34%, Belgium 1%/3%. By the end of the study period, DES were utilised in 75% of stented lesions in the Mayo Clinic, 42% in Scotland, 37% in Alberta and 32% in Belgium.
Conclusion The adoption and use of DES showed wide variation in four countries. The determinants of utilisation are complex, with non-clinical factors predominating such as healthcare payment systems, the role of national regulatory and rationing agencies, clinician autonomy, public and medical perception. Recent reductions in use may be as a consequence of publicity and concerns regarding late stent thrombosis, although surprisingly reductions began before the World Congress of Cardiology meeting in September (widely viewed as an important landmark). No consensus in the optimum application of DES in clinical practice was observed.