Article Text

Abstract
Clinical introduction A 50-year-old woman presented with an inferoposterior ST-elevation myocardial infarction (STEMI) and underwent emergency percutaneous coronary intervention (PCI). Angiography revealed acute occlusion of the circumflex and right coronary (RCA) arteries. PCI was uncomplicated. Her medical history included asthma, hypertension and chronic sinusitis.
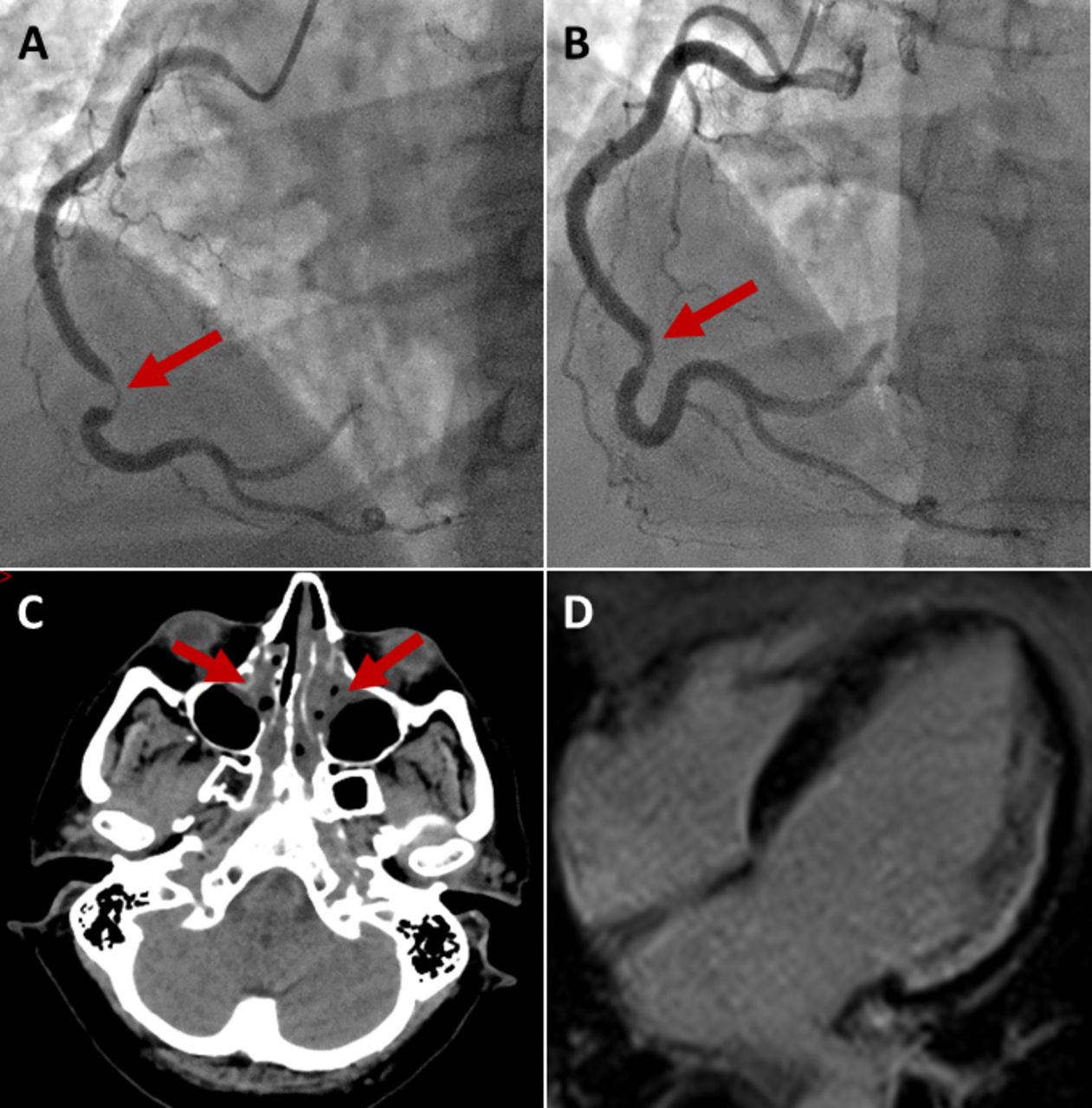
Three months later, she presented with a non-STEMI (NSTEMI), and angiogram showed a new focal stenosis in the left anterior descending artery. Pressure wire assessment induced severe coronary spasm. After liberal intracoronary nitrate, fractional flow reserve measured 0.71, so a further stent was implanted. Six days later, she was readmitted with another NSTEMI. Repeat angiogram revealed patent stents, with severe spasm of the distal RCA which improved following nitrate (figure 1A,B). Four days later, she was readmitted with further NSTEMI. Coronary angiography was not felt to be appropriate, and she was discharged with vasodilator therapy.
{kind=link}
(A) Angiogram of RCA pre nitrates; (B) Angiogram of RCA post nitrates; (C) CT brain post cardiac arrest; (D) CMR post cardiac arrest.
The following day, she had an out-of-hospital ventricular fibrillation (VF) arrest and was successfully resuscitated. CT brain showed no evidence of neurological injury (figure 1C). Cardiac magnetic resonance imaging (CMR) was performed prior to implantable cardioverter defibrillator (ICD) implantation (figure 1D). Eosinophils had been persistently elevated with a peak of 1.78×109 (normal: 0.02–0.5×109). Antinuclear antibodies and antineutrophil cytoplasmic antibodies (ANCA) were negative.
Question?What is the diagnosis for her recurrent acute coronary syndrome and VF arrest?
Aggressive atherosclerotic coronary artery disease.
Prinzmetal’s variant angina.
Loeffler endocarditis.
Coronary vasculitis.
- coronary artery disease
- acute coronary syndromes
- cardiac arrest
Statistics from Altmetric.com
Footnotes
Contributors IM: drafting and submission of manuscript. DC: editing of manuscript and joint guarantor of content. JRD: editing of manuscript and joint guarantor of content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.