Article Text

Statistics from Altmetric.com
Patient-reported outcome measures (PROMs) now are recognised as an essential element in clinical cardiovascular research studies. In addition, we are increasing aware of significant sex differences, not only in risk factors, clinical presentation and outcomes, but in the treatments provided to patients with cardiovascular disease. In this issue of Heart, a study by Gleason and colleagues1 compared atrial fibrillation (AF) therapy and PROMs in women versus men in a cohort of 953 AF patients (mean age 72 years). Overall, women reported more severe AF symptoms, a lower AF-related quality of life, poorer functional status, higher anxiety levels and more symptoms of depression (figure 1); these sex differences persisted even when the type of AF therapy was considered. However, in both men and women, rate control alone was associated with lower functional status and AF-related quality of life compared to a rhythm control strategy.
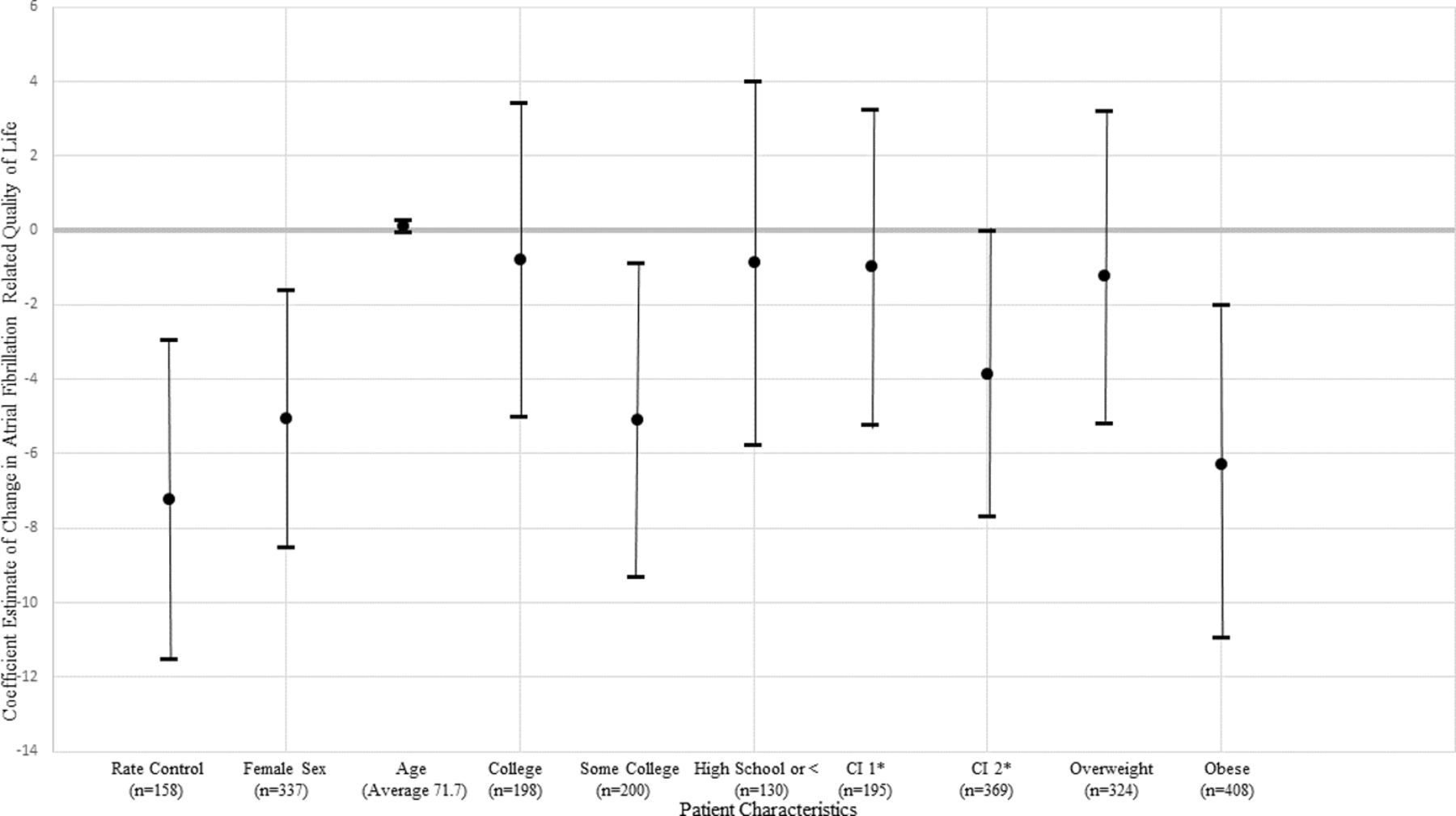
The association of therapies and key patient characteristics with atrial fibrillation-related quality of life in propensity score matched adjust models. Results presented as β, 95% CI. The reference groups for sex, education level, comorbidity index and weight were male sex, greater than college, comorbidity index of 0 and normal weight. *Comorbidity index.
In the accompanying editorial, Hendriks and Strömberg2 remind us that current guidelines for management of AF recommend an integrated care approach in which PROMs are considered and decisions about treatment are made with the patient, not for the patient. They conclude: ‘Given the projected increase in AF prevalence to global epidemic levels in the near future, there is a substantial demand on healthcare services to deliver value-based healthcare. This requires a paradigm shift in which a holistic approach with integration of significant aspects of care is being pursued, in which PROMs should be weighed alongside with gender, symptoms and other clinical parameters, in communication and collaboration with the patient, in order to determine the most optimal and tailored treatment strategy.’
An understanding of the cellular and molecular mechanisms of calcific aortic stenosis (AS) might allow targeted medical therapy to prevent disease initiation and progression. Gomez-Stallons and colleagues3 compared histological patterns of aortic valve leaflet calcification in patients with and without clinical AS. Two distinct phenotypes were identified. Patients with clinical AS typically had ‘nodular’ calcification, extending from the leaflet centre to tips, associated with elastin fragmentation and loss of integrity, corresponding to calcification patterns seen on imaging in patients before transcatheter valve implantation (figure 2). In contrast, valves from adults over age 50 years without clinical AS showed ‘diffuse’ calcification at the leaflet base, with abnormal collagen and proteoglycan deposition, which may not be visible on clinical imaging studies.

Common patterns of aortic valve calcification demonstrated on three-dimensional (3D) contrast-enhanced CT reconstructions of TAVI patients. 3D CT reconstructions are shown as two-dimensional images. (A) Symmetrical and (B) asymmetrical (predominately involving the non-coronary leaflet (N)) regional distribution of nodular calcification is demonstrated in short axis with the most common extent of leaflet involvement observed. In panel (B), the right (R) and left (L) coronary leaflets are less affected, with sparing of the central tip or nodules of Arantius. Panel (B) is then dissected in its long axis (C), again highlighting the extent of the non-coronary leaflet involvement, predominately involving the mid-leaflet (M) and extending to the proximal tip with thickening and sparing of the distal tip (T). There is no involvement of the proximal third or hinge (H) of the leaflet. Higher magnifications are shown in A′–C'. Ao, aorta; LA, left atrium; LV, left ventricle; RA, right atrium; TAVI, transcatheter aortic valve implantation.
Atkins and Aikawa4 point out that research on calcific aortic valve disease (CAVD) increasingly relies on imaging data, rather than histological analysis. ‘Robust studies will allow for the investigation of cell sources contributing to calcification, the mechanisms involved in calcification and the investigation of small molecule inhibitors to block calcification, which will aid in pharmaceutical target development with the goal of inhibiting the onset and progression of CAVD. The combination of in vitro, ex vivo and in vivo analyses with advanced clinical imaging and systems biology will accelerate the rate of target discovery. Systems biology and network analysis can help identify novel pathways involved in CAVD pathogenesis and reveal potential perturbagens to revert abnormal cellular phenotypes’ (figure 3).

(1) Robust in vivo screening combined with radiotracers or near-infrared fluorescent calcium tracer to track the progression of calcific aortic valve disease in high-risk populations (hypertension, diabetes, hyperlipidaemia, bicuspid aortic valve) for early intervention and screening should be performed in parallel with (2) next-generation ‘omics’ techniques that enable collection and study of the entire genome, miRNAome, transcriptome, proteome and secretome. (3) The massive amount of data generated by this multi-omics approach is increasingly being analysed with the aid of artificial intelligence, where machine learning algorithms are employed to identify the most promising drug targets. (4) Target screening performed with in vitro and in vivo models of the pathobiology of interest is used as a first line of investigation. Care is taken to incorporate all relevant cell types, biomechanical stresses, biochemical factors and so on. These models are then used to carefully study the molecular mechanisms which regulate initiation and progression of disease. Once a drug/target has been validated, the cycle will continue again with follow-up patient monitoring and screening using clinical imaging.
Another interesting paper in this issue of Heart 5 found that in patients age 75 years or older with an acute coronary syndrome, cognitive dysfunction identified using a simple bedside test is common (about 1/3 of patients) and is associated with a higher risk of 1 year mortality (adjusted-HR 2.4, 95% CI 1.53 to 3.62, p<0.001), independent of other variables (figure 4). Bellelli and Morandi6 suggest that ‘the assessment of delirium and cognitive function, using appropriate tools, should become a standard of practice in the daily cardiology service. Based on these evaluations, clinicians might be enabled to start specific interventions, such as deprescription of unnecessary drugs, and estimate the benefit:risk ratio before performing invasive procedures in patients with both ACS and cognitive impairment.’
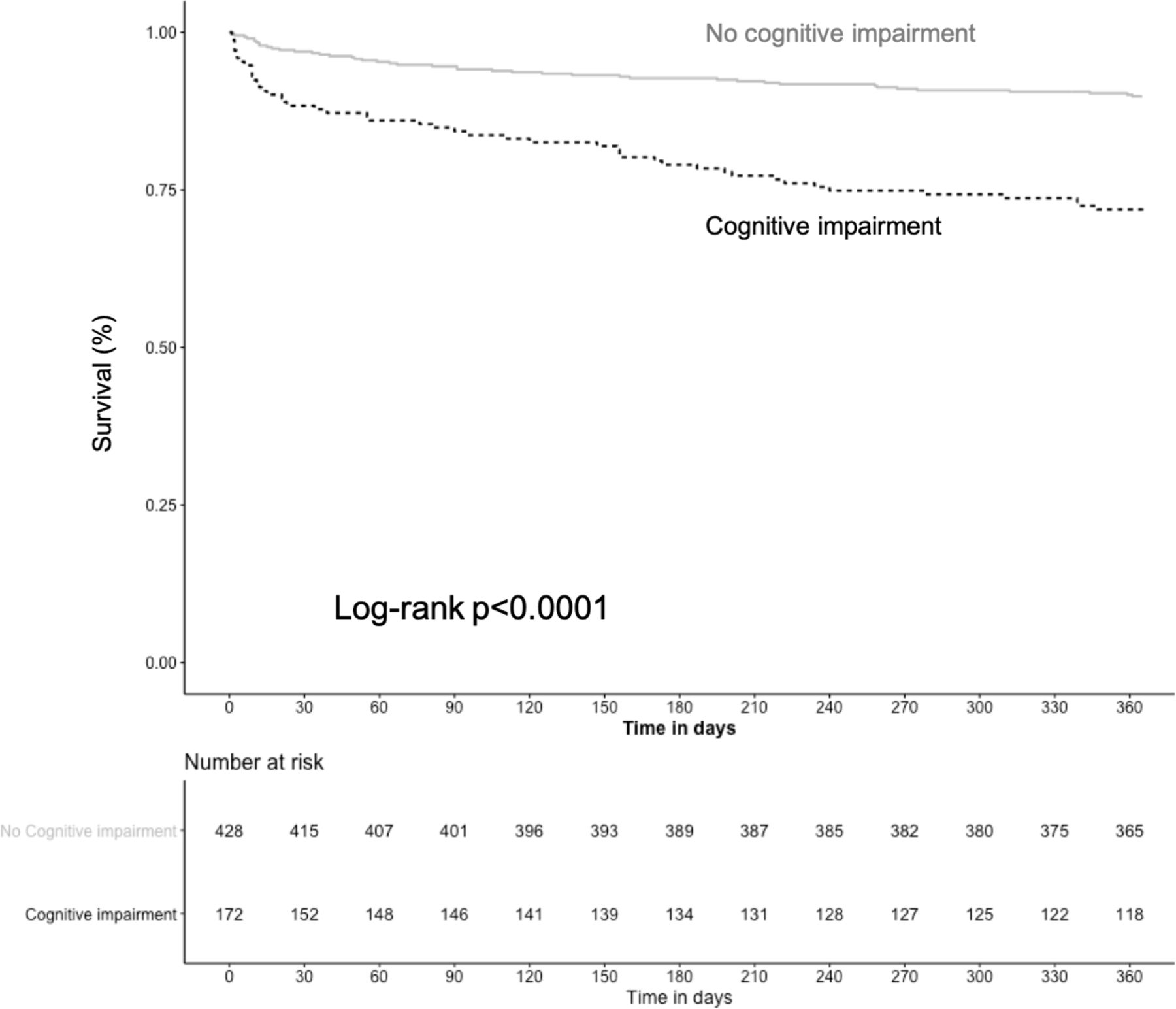
Kaplan-Meier survival curves comparing patients with versus those without cognitive impairment.
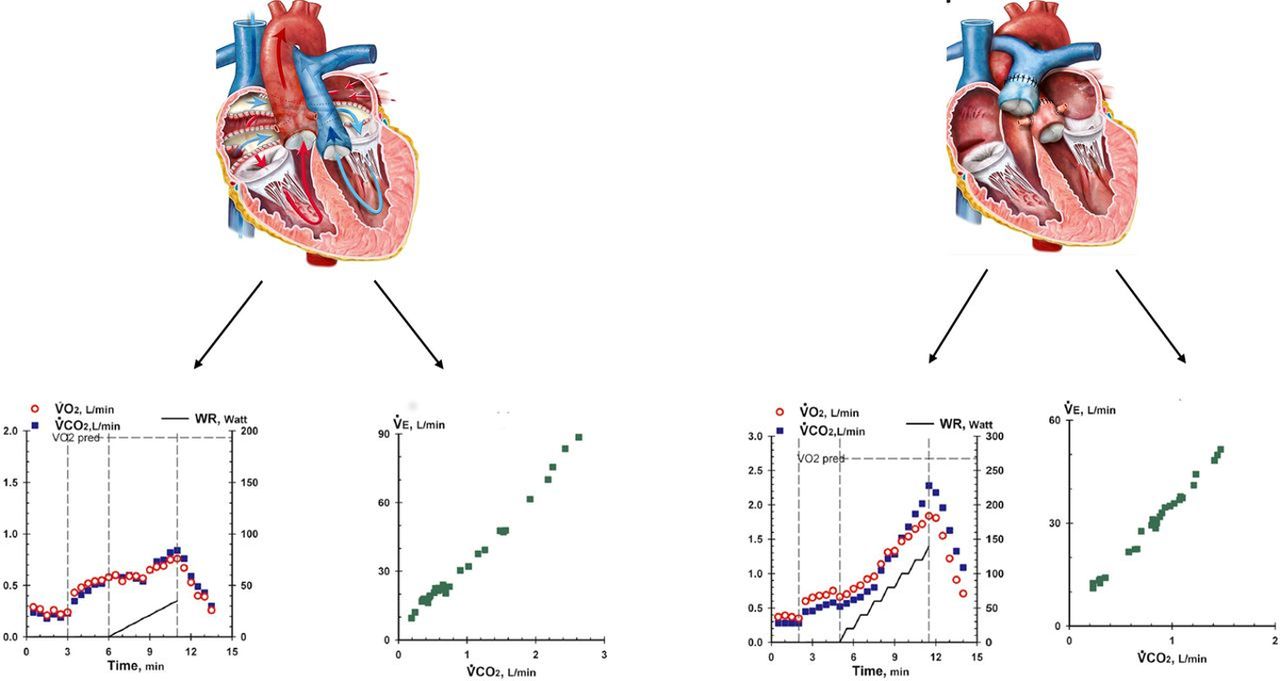
The Education in Heart article in this issue7 summarises the role of exercise testing in adults with congenital heart disease and reviews recommendations for sports participation(figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Theoretical graphical CPET displays of two types of surgeries for D-loop transposition of the great arteries. Left: a patient who is s/p atrial switch operation: intra-atrial baffles redirect systemic venous return to the mitral valve and LV, pulmonary venous return to the tricuspid valve and the right ventricle serves as the systemic pumping chamber. Peak VO2 values (bottom left image) are markedly reduced at about 11 mL/min/kg and the VE/VCO2 slope is markedly elevated at 45 (bottom second from left image, normal: up to 30). Right: a patients who is s/p arterial switch operation: reimplantation of the great vessels at their correct anatomic location, with restoration of the left ventricle as the systemic pumping chamber. Peak VO2 values are nearly normal at 25 mL/min/kg (bottom right image) and the VE/VCO2 slope is normal at 28. CPET, cardiopulmonary exercise testing; LV, left ventricle; VCO2, carbon dioxide production; VE, minute ventilation; VO2, oxygen consumption.
Be sure to try the Image Challenge question8 which is based on an interesting case and unusual findings on CT imaging. Remember that you can access over 100 board review type questions on the Heart webpage (heart.bmj.com) by searching for ‘Image Challenge’ in the search box at the upper right side of the page. Each multiple-choice question is based on a clinical case and image with a detailed explanation of why the correct answer is correct and why the other answers are not. We are always looking for imaging cases with important teaching points or unusual findings; encourage your trainees to submit their own multiple-choice Image Challenge questions.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.