Article Text

Abstract
Background Detection of atrial fibrillation (AF) in patients who had ischaemic stroke and transient ischaemic attack (IS/TIA) is recommended. We aimed to compare external loop recording (ELR) against simultaneous continuous ECG recording for AF detection in patients who had acute IS/TIA and determine sensitivity, specificity and positive predictive value of AF detection using ELR. We hypothesised ELR to detect 15% fewer patients with AF than continuous ECG recording.
Methods In this prospective cohort study, we included 1412 patients who had acute IS/TIA without prior AF. Monitoring was 48 hours. Primary outcome was AF >30 s. Cardiologist verified AF in continuous ECG was gold standard.
Results In continuous ECG, 38 (2.7%) patients had AF. ELR automatically categorised 219/1412 patients (15.5%) with AF, including 32/38 (85%) patients with AF in continuous ECG. After cardiologist adjudication of ELR recordings, AF was diagnosed in 57/219 patients, of which 32 (56%) had AF in continuous ECG. For adjudicated AF detection by ELR, sensitivity was 84%, 95% CI (69% to 94%), specificity was 98%, 95% CI (97% to 99%) and positive predictive value was 56%, 95% CI (42% to 69%).
Conclusion Automatic AF detection with ELR results in an AF diagnosis in more than five patients without AF for each patient with AF as verified in continuous ECG. For adjudicated AF detection by ELR, sensitivity was confirmed to 84% and specificity 98%. Automatic ELR as investigated in this study may be considered to rule out AF, but it is not suitable as a single monitoring device for AF screening in patients early after stroke.
Trial registration number NCT02155907.
- atrial fibrillation
- stroke
Statistics from Altmetric.com
Introduction
Stroke is the second leading cause of death and disability worldwide with 15 million new cases each year.1 It is estimated that 15% of all strokes are caused by atrial fibrillation (AF).2 With a growing elderly population, prevalence of AF increases, and estimated 9% of people older than 65 years have AF.3 AF entails up to five times higher risk of ischaemic stroke and increased risk of recurrent stroke.4 Strokes related to AF cause higher mortality, worse functional outcome and longer hospitalisations.5
It is well documented that oral anticoagulation (OAC) treatment reduces stroke risk significantly in patients with AF,6 and detection of AF in patients who had a stroke is of utmost importance. The paroxysmal and often asymptomatic character of AF is a huge challenge in that setting. Recent guidelines recommend monitoring of 3–30 days in patients who had a stroke to search for AF.7 8 There is, however, no consensus about best method to detect non-persistent AF.
Continuous ECG recording is widely accepted as gold standard in ambulatory heart rhythm analysis. Recently, a considerable range of heart rhythm detection devices have been marketed. External loop recorders (ELRs) hold several practical and economic advantages compared with continuous ECG recording, offering up to 32 days continuous monitoring, high patient comfort and automatic AF-detecting software. Such devices in general are not validated against simultaneous continuous ECG recording in relevant patient cohorts. We aimed to compare 48 hours ELR monitoring against simultaneous continuous ECG recording for AF detection in a large cohort of patients who had a stroke and determine sensitivity, specificity and positive predictive value of AF detection using ELR.
Methods
Prospectively, consecutive patients were recruited from Department of Neurology, Regional Hospital West Jutland in Denmark during June 2013 to December 2017. Inclusion criteria were acute ischaemic stroke or transient ischaemic attack (TIA) with first symptoms within 1 week, age ≥60 years, no AF on 12-lead admission ECG, no prior AF according to International Classification of Diseases codes (ICD-10) from outpatient clinic visits, hospitalisations or review of medical records, no active cancer, no implanted pacemaker, no expected low compliance or precedent participation in this study and written informed consent. Neurologists ascertained diagnosis of stroke or TIA and cerebral imaging (CT or MRI) was obtained for all patients. TIA was defined as stroke-like symptoms lasting shorter than 24 hours. AF was defined according to current guidelines, as an atrial arrhythmia with irregular intervals between R waves, without detectable normal P waves and lasting more than 30 s.9
We started simultaneous continuous ECG recording and ELR monitoring to obtain continuous recording for 48 hours. An illustrating picture is presented in supplementalry appendix 2.
We used R.Test Evolution 4 (NorDiaTech, Paris, France) as ELR. This device is non-invasive and records heart rhythm using two skin electrodes attached over sternum and cardiac apex. ELR recorders were attached by nurses after manufacturer’s recommendations. The ELR analyses segments of 64 consecutive RR intervals (intervals between R waves), when at least two-thirds of these intervals are irregular, categorises heart rhythm as AF and stores a recording of AF episode in memory. Depending on heart rate, the ELR is able to categorise AF episodes lasting from approximately 25 s, thereby suitable for detecting AF exceeding 30 s. Storing capacity is 60 min, and if this is exceeded, only the most characteristic AF episodes are kept. AF episodes with fastest heart rates are kept in memory. We adjusted ELR according to manufacturer’s recommendations. We saved 1 min recording per AF episode, allowing for a maximum of 54 AF recordings per patient, while 6 min were spared for storage of episodes of other arrhythmia.
Three experienced members of the research team (MHS, OM and JCN) each reviewed and classified as AF or non-AF all recordings automatically classified as AF by the ELR. In case of ambiguity, agreement was reached by consensus. Analysis of ELR findings was blinded for continuous ECG recording results. The continuous ECG recorder used was Life Card CF digital ECG recorder from Spacelabs Healthcare Diagnostic Cardiology (Washington, USA). Nurses trained and experienced in analysing continuous ECG recordings reviewed recordings. Episodes classified as AF were verified by the three members of the research team. Analysis was blinded to ELR results.
Ethics
The study complies with Declaration of Helsinki and was reported to ClinicalTrials.gov.
Statistical analysis
Baseline and follow-up data were presented as numbers (percentages) and means (SD) if normally distributed; otherwise, data were presented as median (IQR). We used STATA V.15 from StataCorp LP for statistical analyses.
Continuous ECG recording was defined as gold standard as we aimed to estimate sensitivity, specificity and positive and negative predictive values of AF detection using ELR, both for automatically detected AF and after review of AF episodes by experienced cardiologists. Detection of AF was categorised as binary outcome.
We used the DIAGT Stata V.15 module to report sensitivity, specificity, positive predictive value and negative predictive value from our contingency tables (table 2), all with exact binomial confidence intervals. Here we compared AF in continuous ECG to AF registered in ELR recordings, as well as AF in continuous ECG to validated AF in ELR. AF in continuous ECG was set as gold standard in the STATA command.
Ischaemic stroke: includes the ICD-10 diagnosis codes: DI639, DI649, DI632, DI453 and DI634
Sensitivity, specificity, positive and negative predictive values of automatically detected and cardiologist verified AF detection by ELR with 95% CI compared with findings with 48 hours continuous ECG recording as gold standard
We expected 48 hours continuous ECG recording to detect AF in 10% and ELR in 8.5% of patients, thus expecting a sensitivity of 85%.10
Hypothesis: 2-day ELR has a sensitivity of 85% compared with 2-day continuous ECG recording (gold standard) to detect AF in a consecutive population with recent stroke/TIA.
Null hypothesis: 2-day ELR sensitivity differs from 85% compared with 2 day continuous ECG recording (gold standard) in a consecutive population with recent stroke/TIA.
Sample size
We estimated a required sample size of 1480 patients in order to detect an ELR sensitivity difference of at least 10% from a hypothesised sensitivity of 0.85, assuming detection of AF in 10% of the population. A binomial (two sided) test comparing one proportion (the sensitivity of 0.85) to a reference value (0.75) was used. A priori, sample size was not calculated for specificity comparisons.
Results
Flow diagram depicting numbers of patients who had ischaemic stroke and TIA older than 60 years hospitalised in our department during the inclusion period is shown in figure 1. We included 1507 patients consecutively. We excluded 95 patients, in whom ELR recording was not started correctly, resulting in a study cohort of 1412 patients with simultaneous 48 hours ELR and continuous ECG recording. Baseline characteristics of study cohort is presented in table 1. Eight hundred and forty-nine patients (60.2%) had ischaemic stroke and 562 patients (39.8%) had TIA. Median (IQR) ELR monitoring time was 48.2 (1.55) hours with duration of analysable recording of 45.1 (14.3) hours. Duration of analysable continuous ECG recordings was 48.0 (1.08) hours.
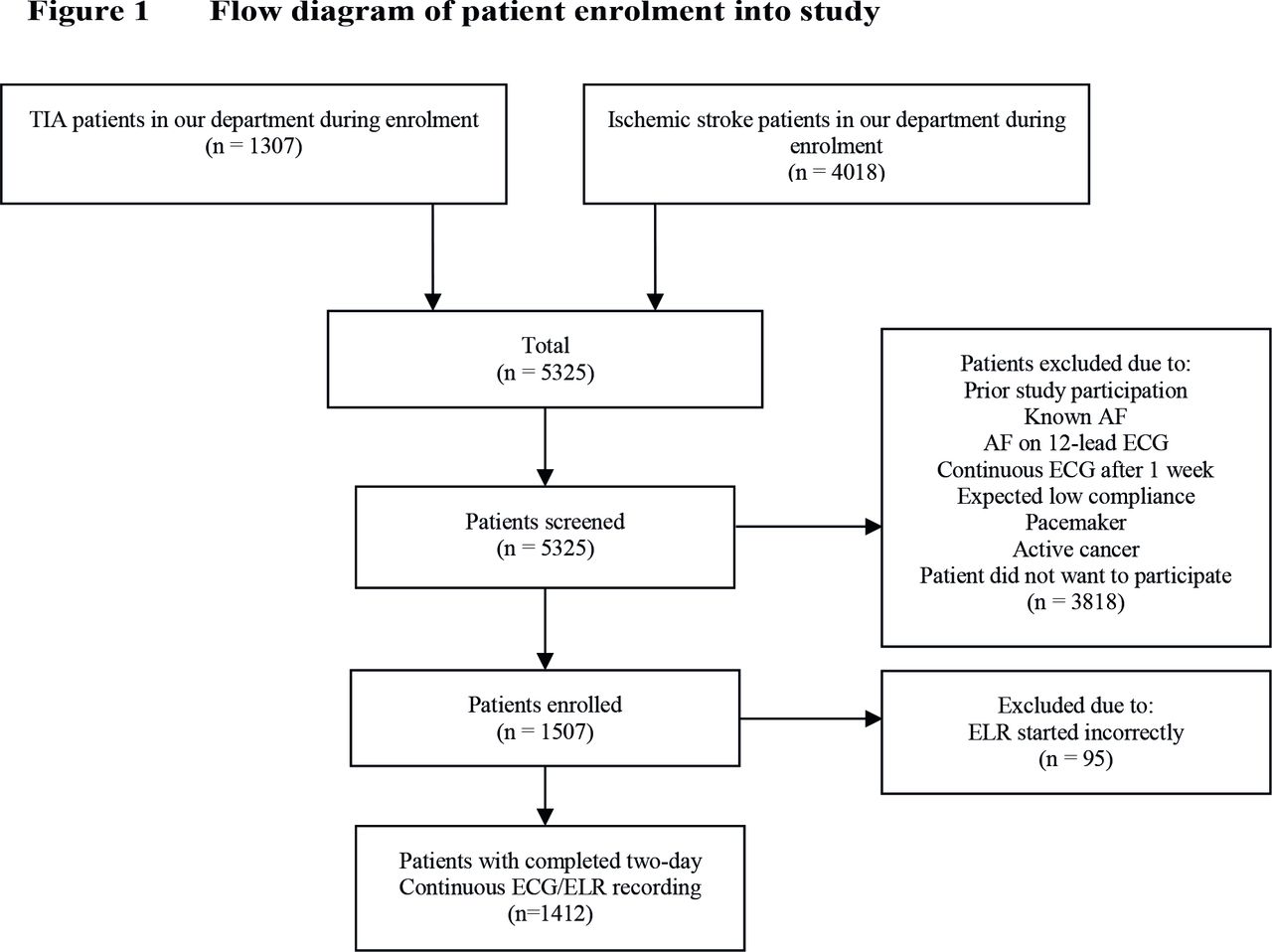
Flow diagram depicting numbers of patients older than 60 years hospitalised with ischaemic stroke or TIA during inclusion period. ELR, external loop recorder; TIA, transient ischaemic attack.
The ELR automatically categorised 219 of the 1412 patients (15.5%) with AF. The 219 ELR recordings were reviewed by trained cardiologists among the authors and 57 (26.0%) were verified as AF, while remaining 162 (74.0%) were classified as non-AF. AF detected by ELR and verified by cardiologists was prevalent in 4.0% (57/1412) of patients. In continuous ECG recording, we detected AF in 38 patients, corresponding to a prevalence of 2.7% (38/1412). Automatically, ELR detected 12.8% (95% CI 11.0% to 14.7%) more patients with AF than did continuous ECG recording. After cardiologist’s adjudication of AF episodes from ELR, AF prevalence was 4.0% (57/1412), and ELR detected 1.3% (95% CI 0.50% to 2.1%) more patients with AF than continuous ECG recording.
Discrepancies between the two monitoring methods’ findings are illustrated in figure 2. Of the 38 patients with AF in 48 hours continuous ECG recording, 32 were detected and verified as AF on ELR. The remaining six had either no AF detection in ELR (three patients) or had AF events recorded in ELR that were disproved by the authors and did not match time of AF on continuous ECG recording (three patients). AF durations on continuous ECG for those six patients were: 54, 80, 123, 218, 23 476 and 64 140 s, respectively. Sensitivity and specificity of AF detected by ELR automatically and as verified by cardiologists are presented in table 2.

Flow diagram illustrating results of AF diagnostics in continuous ECG and ELR. Green marked boxes represent patients with AF in continuous ECG. AF, atrial fibrillation; ELR, external loop recorder.
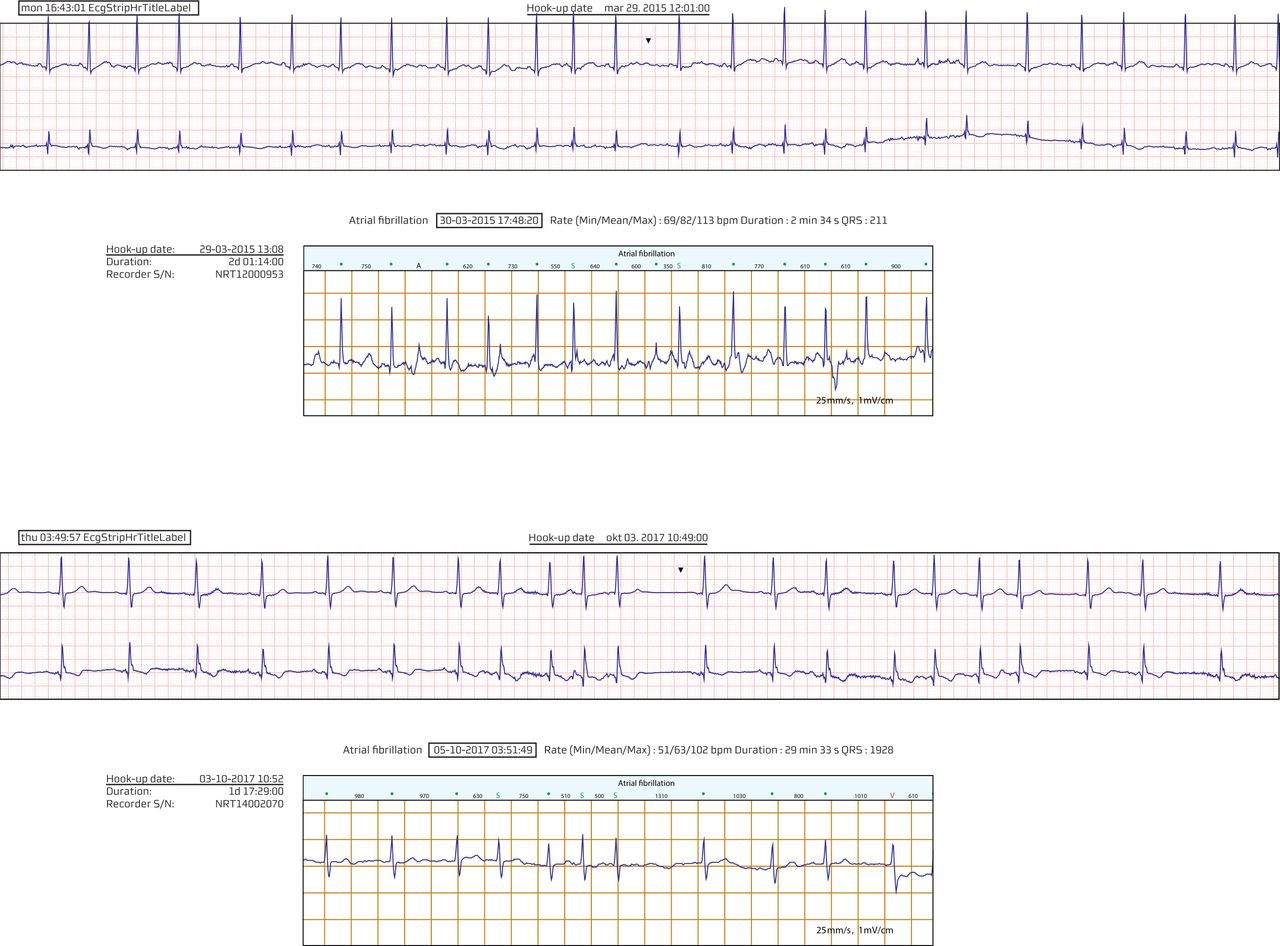
For the 25 patients recognised discordantly with non-AF in continuous ECG and AF in ELR, rhythm in ELR recording did fulfil AF criteria of irregular heart rhythm with no detectable P waves and duration longer than 30 s. We reviewed simultaneous two-channel continuous ECG recordings during the relevant periods with AF in ELR. For all 25 cases, we were able to identify P waves during the entire continuous ECG recording, confirming sinus rhythm with premature atrial complexes. These 25/57 (43.9%) ELR recordings therefore turned out falsely positive. Figure 3 presents some simultaneous ELR and continuous ECG recordings with discordant results; remaining simultaneous recordings are shown in online supplementary appendix 1. Figure 4presents two patients with AF in continuous ECG recording not detected by ELR. Considering automatic AF detections by ELR, these were truly positive in only 14.6% (32/219) of patients and thereby false positive in 85.4% of patients (table 2). Mean AF duration in ELR was shorter in the 25 patients where AF could not be confirmed in continuous ECG recording (1 hour 1 min 7 s) than in the 32 patients with confirmed AF (11 hours 56 min 17 s) (online supplementary appendix).
Supplementary file 1
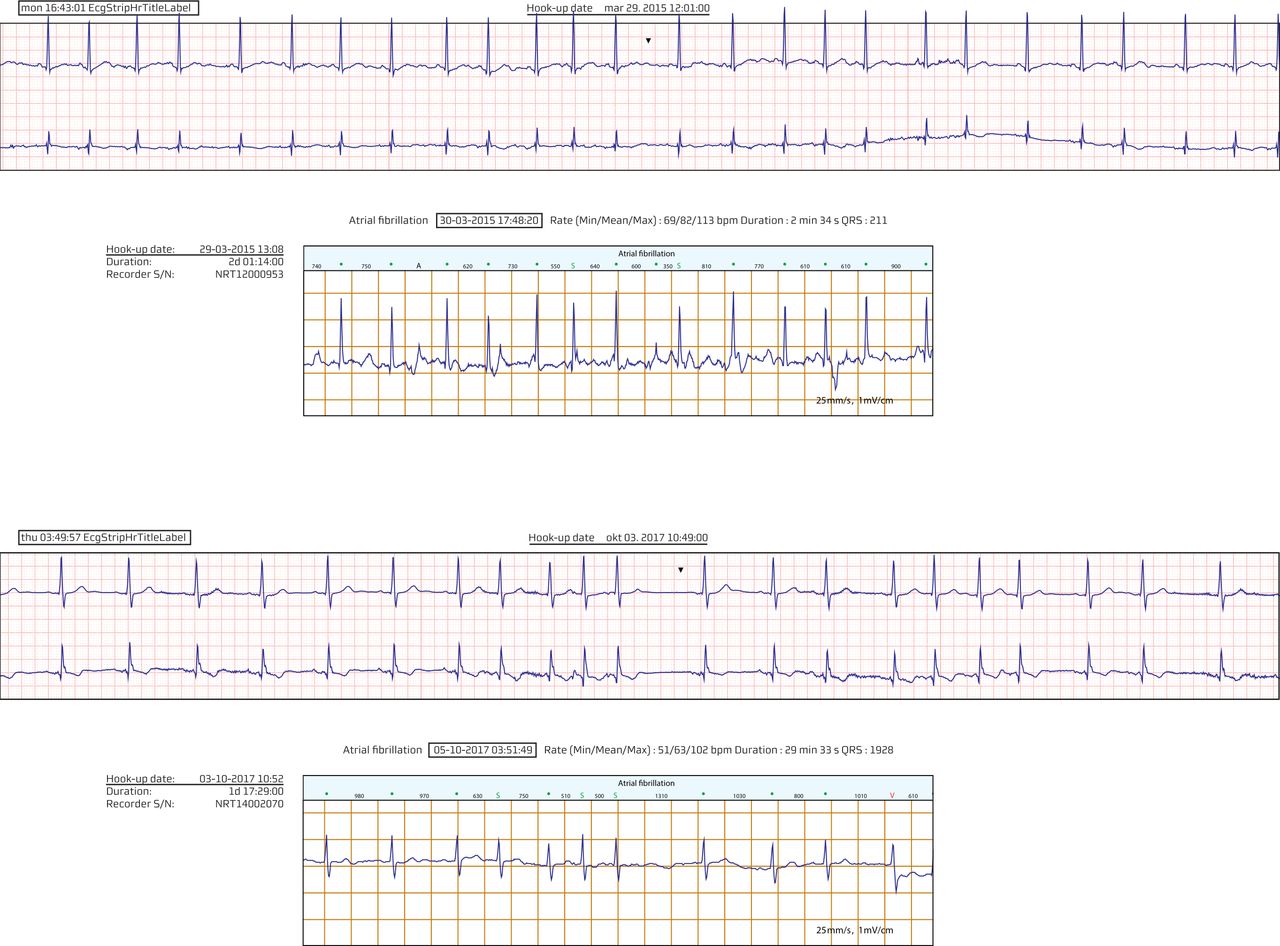
Examples of simultaneous 48-hour continuous ECG (top) and ELR (bottom) recordings from patients adjudicated as AF by experienced cardiologists among the authors but confirmed as sinus rhythm with supraventricular extra systoles in simultaneous 48-hour continuous ECG recording. Recorded time of AF and hook-up time are marked for all tracings. The 48-hour continuous ECG recording clock was set manually, while ELR runs at exact computer time from encoding. Some recordings have approximately 1-hour time difference since the manual 48-hour continuous ECG recording setting was not corrected to winter time. AF, atrial fibrillation; ELR, external loop recorder.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A and B) Two of six patients diagnosed with AF on 48-hour continuous ECG recording but missed by ELR. AF, atrial fibrillation; ELR, external loop recorder.
Discussion
This study shows that results obtained by ELR monitoring differed markedly from results obtained by the gold standard method of continuous ECG recording while screening for AF in patients who had an acute stroke. Automatic ELR detection of AF results in an AF diagnosis in more than five patients without AF for each patient with continuous ECG recording-verified AF. For adjudicated AF detection by ELR, sensitivity was confirmed to 84% and specificity 98%. Automatic ELR as investigated in this study may be considered to rule out AF, but it is not suitable as a single monitoring device for AF screening in patients early after stroke.
Our population is representative for patients with stroke or TIA admitted to hospital and represents a population where screening for AF is recommended.7 The observed AF prevalence of 2.7% in 48-hour continuous ECG recording is consistent with AF diagnosed in 1%–5% using 24–48 hour continuous ECG recording of stroke patients reported in a recent review.11 The high rate of false-positive detections of AF with ELR is accordant with findings in three small studies comparing ELR with simultaneous ECG recording.12–14 This finding indicates that in patients who had an acute stroke, clinicians should not rely on a diagnosis of AF established only by ELR monitoring. Not even after cardiologist verification of these recordings, as only 56% of such findings truly reflect AF.
We found that ELR detected 85% of the patients who had true AF as indicated by continuous ECG monitoring. The negative predictive value of ELR was high, and therefore, this monitoring device may be considered as a first-line instrument in screening patients who had an acute stroke for AF. However, in case AF is indicated by ELR, this diagnosis should be confirmed by continuous ECG monitoring or another more reliable AF detection method before clinical consequences as initiation of OAC treatment are taken.
The main reason for false-positive AF detections in the present study was automatic ELR rhythm interpretation relying on RR intervals. We included elderly patients who had a stroke/TIA, and both ageing and prior stroke are associated with increased prevalence of premature atrial and ventricular contractions.15 Premature beats are known to be even more frequent very early after stroke,16 and it cannot be ruled out that later monitoring would yield different results. One reason that continuous ECG recording is more reliable than loop recorders may be heart rhythm evaluation during the entire recording period, allowing for diagnostic identification of gradual or abrupt changes in atrial and ventricular rates.
OAC therapy is documented highly beneficial in stroke patients with AF reducing risk of recurrence.6 17 However, anticoagulation therapy comes with an enhanced risk of bleeding and intracranial bleeding, especially in patients with earlier stroke or TIA.18 Using less reliable methods for AF detection may lead to OAC in patients without AF. These patients are exposed to risks with OAC, but likely no benefit of reduced stroke risk, as supported by the recent Navigate ESUS study results.19
There are no generally accepted international guidelines on optimal duration and method of rhythm monitoring for AF detection in patients who had a stroke. We started patient inclusion in 2013. Since 2008, the European Stroke Organization recommended 24-hours continuous ECG monitoring in acute ischaemic stroke patients and additionally 24-hour continuous ECG recording for selected patients.20 Our monitoring strategy is according to these recommendations. In 2016, European Heart Rhythm Association and European Stroke Organisation recommended screening for AF in patients who had an ischaemic stroke or TIA by short-term ECG recording followed by continued ECG monitoring for at least 72 hours.7 Several studies published within recent years encourage longer monitoring time of patients who had a cryptogenic stroke since it reveals significantly more AF events. The American Heart Association recommends 30-day monitoring of patients who had a stroke since 2014.8
It is not straightforward to offer 30-day continuous ECG recording for all patients who had a stroke. This would necessitate major resources for manual analysis of recordings. Most continuous ECG recording devices in use are not capable of such long-time recording. Incidence of skin reactions from wearing continuous ECG recording electrodes is not negligible. In 2014, Tu et al 21 reported that 28-day continuous ECG recording was poorly tolerated in patients who had a cryptogenic stroke, with only 40% completing the recording period; remaining patients were excluded mainly due to skin irritation and also artefacts caused by loose electrodes and trouble sleeping with the device caused exclusions. Higher patient comfort and compliance was observed with a specially designed textile wearable continuous ECG recorder, resulting in 84% of patients who had a cryptogenic stroke completing 28-day recording.22 Gain of prolonging continuous ECG recording in AF detection is currently explored in the ongoing German Impact of standardized MONitoring for Detection of Atrial Fibrillation in Ischemic Stroke trial.23
Considering American guidelines, automatically detecting ELR devices are attractive alternatives to continuous ECG recording, being able to record for 30 days, associated with less patient discomfort and less costly to analyse. However, the type of ELR used must identify AF reliably. For longer term monitoring, implantable loop recorders are superior with respect to patient comfort and reliability24 but more expensive and requiring surgery. Documenting cost-effectiveness of ILR in patients who had a stroke is still needed. Ambulatory telemetry has been tested only in small cohorts25 and requires personnel validating the results manually. Prolonged inpatient telemetry has been studied and results in higher rates of AF detection in patients who had a stroke.26 However, in Denmark, the average patient who had a stroke is admitted to hospital for 2 days and patients who had a TIA even shorter. A wealth of different devices recording heart rhythm is being marketed: mobile phones, thumb-ECG, earlobe sensors, smartwatches and automated blood pressure monitors. For such devices, performance should be tested before using for screening patients who had a stroke.
Study strengths
The essential strength of this study is simultaneous ELR monitoring and continuous ECG recording in patients who had an acute stroke and TIA, permitting true validation of ELR against the gold standard of continuous ECG recording. A large number of patients were included, allowing for more reliable statistical estimates. Investigators analysing continuous ECG recordings were blinded to ELR tracing results and vice versa. The study was performed in Denmark where the healthcare system is free of charge. All Danish patients who had a stroke and TIA are referred to neurological departments and treated according to national and European guidelines without regard to social and economic status. Therefore, the patients represent an unselected stroke population and the results are considered generalisable.
Study limitations
Not all patients consented, and few patients were not asked because low compliance was anticipated. In periods of high occupancy, we had shortage of continuous ECG recorders and not all patients could be included. It is, however, not likely that inclusion of these patients would have changed the comparison between ELR and continuous ECG recordings. We excluded 95 patients with ELR started incorrectly, resulting in empty recordings. As ELR recordings are not real-time transmissions, quality of recording could not be controlled until after detachment of device. An ELR recorder easier to use might have reduced this problem. Planning the study, we expected AF prevalence of 10% in 48-hour continuous ECG, but we observed a prevalence of 2.7%. This discrepancy should be taken into account interpreting positive predictive value and negative predictive value reported, as accuracy of both decreases with more rare observations. Furthermore, we did not calculate our sample size for specificity.
The ELR tested in this study used only single-lead recording from two electrodes. Using another type of ELR recording with more than one lead may have allowed better differentiation between AF and non-AF rhythms. We used the generally accepted definition of AF at 30 s duration. It cannot be ruled out that the ELR may have performed better with respect to properly detecting longer AF episodes.
Summary
Automatic AF detection with ELR results in an AF diagnosis in more than five patients without AF for each patient with AF as verified in continuous ECG. For adjudicated AF detection by ELR, sensitivity was confirmed to 85% and specificity 98%. Automatic ELR as investigated in this study may be considered to rule out AF, but it is not suitable as a single monitoring device for AF screening in patients early after stroke.
Therefore, this type of automatic ELR, however, is not suitable.
The author group has no economic interest in the research results and received no financial support from ECG recorder or ELR provider. The corresponding author has the right to grant on behalf of all authors and does grant on behalf of all authors an exclusive licence on a worldwide basis to the BMJ Publishing Group Ltd (BMJPGL) and its licencees to permit this article to be published in Heart and any other BMJPGL products to exploit all subsidiary rights.
Key messages
What is already known about this subject?
It is well documented that oral anticoagulation treatment reduces stroke risk significantly in patients with atrial fibrillation (AF) and detection of AF in patients who had a stroke is of utmost importance.
There is, however, no consensus about best method to detect non-persistent AF.
What might this study add?
Automatic AF detection with external loop recorder (ELR) results in an AF diagnosis in more than five patients without AF for each patient with AF as verified in continuous ECG. For adjudicated AF detection by ELR, sensitivity was 84%, positive predictive value was 56% and specificity was 98%.
How might this impact on clinical practice?
Automatic ELR as investigated in this study may be considered to rule out AF, but it is not suitable as a single monitoring device for AF screening in patients early after stroke.
Supplementary file 2
Acknowledgments
We would like to thank nurses at our Department of Neurology, especially Ida Tølbøl, Anette Smidth, Birgitte Brøgger, Mette Jensen; nurses at Department of Cardiology: Marie Jensen, Britta Graversen, Helle Schlosser, Ruth Larsen, Birgit Pedersen and Mette Mark; and Mads Liseborg on graphics.
References
Footnotes
Contributors MHS contributed in literature search, fund applications and obtaining permits, figures, study design, data collection, data analysis, data interpretation and writing. JCN contributed in literature search, figures, study design, data analysis, data interpretation, writing and guidance on cardiological aspects. OM contributed in figures, study design, data interpretation, writing and guidance on cardiological aspects. DD contributed in study design, writing and guidance on neurologic aspects. BFS contributed in data collection, writing and guidance on neurologic aspects.
Funding This work was supported by Health Research Fund of Central Denmark Region (1-31-72-15-14), Danish Heart Foundation (14-R97-A5075-22884/17-R115-A7606-22069) and Aase and Ejnar Danielsen Foundation (10-001847). Novo Nordisk Foundation (NNF16OC0018658) and an institutional unrestricted grant from Abbott, Denmark, supported JCN.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.