Article Text

Abstract
Objectives (1) Describe how the risk of major adverse cardiovascular events (MACE) in individuals with chronic myeloid leukaemia (CML) has evolved; (2) evaluate the risk of MACE associated with the prescription of different CML tyrosine kinase inhibitors (TKI).
Methods A population-based retrospective study including all patients (n=4238) diagnosed with CML in Ontario, Canada between 1986 and 2017 and and age-matched and sex-matched individuals who received healthcare but who did not have CML (controls: n=42 380). The cohort was divided into those entering before 2001 vs from 2001 onwards (when TKIs were introduced). We developed competing risks models to compare time-to-event in CML cases versus controls. We adjusted for baseline comorbidities and present subdistribution HRs and 95% CIs. The relationship between TKI use and MACE was assessed by logistic regression.
Results Before 2001 and from 2001 on, patients with CML had a higher crude incidence of MACE than patients without CML (19.8 vs 15.3 and 20.3 vs 12.6 per 1000 person-years, respectively). After adjustment for cardiovascular risk factors, patients with CML had a lower subdistribution hazard for MACE (0.59, 95% CI 0.46 to 0.76) before 2001; but from 2001, the adjusted subdistribution HR for MACE (1.27, 95% CI 0.96 to 1.43) was similar to age-matched and sex-matched patients. The incidence (9.3 vs 13.8 per 1000 person-years) and subdistribution hazard for cardiovascular death (0.43, 95% CI 0.36 to 0.52) were lower in patients with CML than controls before 2001. From 2001 on, the incidence (6.3 vs 5.4 per 1000 person-years) and subdistribution hazard for cardiovascular death (0.99, 95% CI 0.84 to 1.18) were similar to age-matched and sex-matched patients without CML with a higher risk of cerebrovascular events (8.6 vs 5.6 per 1000 person-years; 1.35, 95% CI 1.00 to 1.83) and peripheral arterial events (6.9 vs 3.0 per 1000 person-years; 1.66 95% CI, 1.15 to 2.39) in patients with CML than patients without CML. Compared with imatinib, there was no difference in the risk of MACE among those prescribed dasatinib (OR 0.67, 95% CI 0.41 to 1.10) or nilotinib (OR 1.22, 95% CI 0.70 to 1.97).
Conclusions In a contemporary CML population, the risk of MACE and cardiovascular death is at least as high as among age-matched and sex-matched patients without CML and may be higher for cerebrovascular and peripheral arterial events. No difference in the risk of MACE between imatinib, dasatinib and nilotinib was observed.
- epidemiology
Statistics from Altmetric.com
Introduction
Chronic myeloid leukaemia (CML) is a myeloproliferative neoplasm caused by the constitutive activation of the BCR-ABL1 oncogene. Untreated, CML progresses to a blast phase, which has a median survival of 3–12 months.1 CML was the first malignancy for which effective targeted therapies were developed. Although BCR-ABL tyrosine kinase inhibitors (TKIs) dramatically improve survival in CML, their chronic use potentially exposes patients to adverse off-target drug effects. In particular, there have been reports of an increased risk of major adverse cardiovascular events (MACE), with the newer TKIs.2 The incidence of MACE in patients receiving TKIs for CML remains uncertain, however. With the reduction in CML death seen following the advent of TKIs over the past two decades, MACE may now represent an important cause of morbidity and mortality among patients with CML. Therefore, we conducted a population-based cohort study with the following objectives:
Compare the risk of MACE and cardiovascular mortality in a cohort of patients with CML with that of a population cohort matched for age and sex.
Evaluate the impact of the implementation of TKIs on the risk of MACE and cardiovascular death among patients with CML by comparing the risk of these outcomes in a cohort of patients diagnosed with CML before and a cohort diagnosed after the introduction of TKIs.
Compare the risk of MACE in patients with CML receiving treatment with different TKIs.
Methods
We conducted a retrospective cohort study in which we included patients aged ≥18 years diagnosed with chronic phase CML in Ontario, Canada between January 1986 and January 2017. Ontario has over 14 million residents who have access to publicly insured healthcare. Eligible patients were identified from the Ontario Cancer Registry, which contains individuals diagnosed with a malignancy from 1964 onwards. All patients with CML were included. Patients entered the study at the time of their CML diagnosis. Patients were linked to other population-based health administrative databases to which the Institute of Clinical and Evaluative Sciences (ICES) has access. These datasets were linked using unique encoded identifiers. These included the Ontario Drug Benefit programme, from which we obtained data on prescriptions dispensed for TKIs. The Ontario provincial government insures the cost of TKIs for adults aged ≥65 years. For patients aged <65 years, access to TKIs requires either private health insurance, the patient to pay out-of-pocket or access to a compassionate drug scheme. Each CML patient was age-matched and sex-matched using greedy nearest neighbour matching with 10 controls without CML. Controls were drawn at random from individuals who had an encounter of any type with the Ontario healthcare system but who had no history of CML. Matching was stratified by entry into the cohort before 2001 vs 2001 onwards.
The primary outcome was MACE, defined as hospitalisation for myocardial infarction, cerebrovascular disease or peripheral arterial disease. Relevant hospitalisations were identified from the Canadian Institute for Health Information Discharge Abstract Database, in which hospital discharges and associated International Classification of Diseases (ICD) codes are recorded (online supplemental appendix). For the primary analysis, we included any outcome event reported as a diagnostic code during a patient’s hospitalisation. In a sensitivity analysis for the MACE outcome, we only considered hospitalisations where the diagnostic codes of interest were either most responsible for length of stay, pre-admission comorbidities that contributed to length of stay or a postadmission comorbidity that contributed to length of stay. The secondary outcome was cardiovascular death, as recorded by the physician certifying the patient’s death.
Supplemental material
Statistical analysis
Comparisons between categorical variables were performed using the χ2 test. Time-to-event was displayed by cumulative incidence curves.3 Patients with CML are susceptible to death from their underlying malignancy, therefore, non-cardiovascular death is a competing risk for cardiovascular death and MACE. We constructed time-to-event models by Cox proportional hazards models for mortality and by competing risks regression for all other outcomes.4 Competing risks regression models estimate the risk of MACE and cardiovascular death under the assumption that if an individual dies of non-cardiovascular causes, they remain in the at-risk pool when estimating the hazard for MACE or cardiovascular death. The time scale used for competing risks models was patient’s age. To preserve patient privacy, we did not have access to exact patients’ ages, only age strata; we assumed each patient’s age was the median value of their stratum. For competing risks models, subdistribution HRs with 95% CIs are presented and adjustment was made for age, sex, history of hypertension, diabetes, myocardial infarction, cerebrovascular disease, peripheral arterial disease, heart failure, chronic obstructive pulmonary disease and rural versus urban location. History of myocardial infarction, cerebrovascular disease and peripheral arterial disease were identified from hospital admissions data by using the same ICD codes as for the MACE outcome if the relevant hospital admission with these diagnoses occurred before the date of study entry. History of hypertension,5 diabetes,6 heart failure7 or chronic obstructive pulmonary disease8 was determined from databases including Canadian Institute for Health Information Discharge Abstract Database, the Ontario Health Insurance Plan and the Same Day Surgery Database using algorithms that have previously been validated. We performed sensitivity analyses in which models were repeated after excluding individuals with a history of myocardial infarction, cerebrovascular disease, peripheral arterial disease or heart failure.
Owing to the reduction in CML-mortality attributable to TKI use, we performed analyses stratified by whether the patient entered the cohort prior to 2001 (ie, when imatinib use began in Ontario) versus from 2001 onwards. We evaluated whether the relationship between CML and outcome events differed prior to versus from 2001 by a statistical test of interaction. Following the approval of imatinib for use in Canada in 2001, the other TKIs were approved by Health Canada and subsequently funded by the Ontario government at various times, with dasatinib approved in 2007, nilotinib approved in 2010, bosutinib approved in 2014 and ponatinib the most recently approved (in 2015) and funded (in 2017).
To evaluate the relationship between the use of specific individual TKIs and the occurrence of cardiovascular events, we adopted an approach that accounted for instances when a patient changed from one TKI to another. In the event that an outcome event occurred following a patient’s last recorded dispensation of TKI, we considered the outcome event to be related to the TKI if it occurred within 1 year of the most recent TKI dispensation. We used logistic regression to model the relationship between TKI use and the occurrence of MACE. The model was adjusted for the length of time each patient was prescribed each individual TKI as well as a past history of hypertension, diabetes, myocardial infarction, cerebrovascular disease, peripheral arterial disease, heart failure and chronic obstructive pulmonary disease.
For all analyses, α was set at 0.05 and analyses were conducted using STATA V.16.1 (College Station, Texas, USA).
Results
Patients with CML versus controls
We identified 4238 patients with CML and 42 380 age-matched and sex-matched controls without CML. Their baseline characteristics are presented in table 1. Patients with CML had a higher baseline prevalence of cardiovascular risk factors (hypertension and diabetes), cardiovascular disease (including previous myocardial infarction, cerebrovascular disease, peripheral arterial disease), heart failure and chronic obstructive pulmonary disease than controls. When the cohort was divided in those entering before 2001 vs 2001 and after, the higher prevalence of diabetes and cardiovascular disease among patients with CML as compared with controls was observed in both time periods.
Baseline characteristics of chronic myeloid leukaemia (CML) cases and of controls
Time-to-event models in patients with CML and controls
Time-to-event analyses are presented in table 2. During a median follow-up of 8.6 years, 2215 (52%) individuals with CML and 12 597 (30%) controls died.
Models comparing patients with chronic myeloid leukaemia (CML) with controls adjusted for history of myocardial infarction (MI), cerebrovascular disease, peripheral arterial disease (PAD), heart failure, diabetes, hypertension, chronic obstructive pulmonary disease, rural location presented overall and stratified by entry into the database before 2001 vs 2001 or later
During follow-up, among those with CML, 614 (14%) developed MACE; 296 (7%) died from cardiovascular causes and 1919 (45%) died of non-cardiovascular causes. Among those with CML dying of non-cardiovascular causes, 1598 died without having experienced a MACE. Among controls, 6202 (15%) developed MACE; 4226 (10%) died of cardiovascular causes and 8371 (20%) controls died of non-cardiovascular causes. Among controls dying of non-cardiovascular causes, 6166 died without having experienced MACE.
Compared with controls, the adjusted subdistribution HR (95% CI) for cardiovascular death among patients with CML was 0.66 (0.58 to 0.75) and the adjusted subdistribution HR (95% CI) for MACE was 0.88 (0.75 to 1.03). The risk of myocardial infarction was lower among patients with CML than controls, with adjusted subdistribution HR (95% CI) 0.76 (0.60 to 0.97). There was no difference in the risk of a cerebrovascular event or a peripheral arterial disease event, with respective adjusted subdistribution HRs (95% CI) 0.86 (0.67 to 1.10) and 1.23 (0.92 to 1.65).
Outcomes before versus after 2001
Crude outcome event incidence rates are presented in table 3 and adjusted HRs for death and adjusted subdistribution HRs for cardiovascular death, MACE and its components in CML cases as relative to controls are presented in table 2. Before 2001, crude mortality rates were higher among patients with CML than controls. Mortality rates among both patients with CML and controls fell from 2001 as compared with before 2001; however, the proportionate reduction in mortality was larger among patients with CML so that the risk of death among patients with CML (relative to controls) was significantly lower from 2001 onwards (coinciding with the introduction of TKIs in Ontario) as compared with pre-2001 (interaction p<0.0001).
Crude incidence rates of mortality, cardiovascular (CV) death and major adverse cardiovascular events (MACE), where MACE included myocardial infarctions (MI), cerebrovascular events and peripheral arterial disease (PAD) events
Before 2001, crude cardiovascular mortality rates were higher among controls than among patients with CML. From 2001, there was a larger proportionate reduction in cardiovascular mortality among controls than among patients with CML. The subdistribution HR for cardiovascular death differed before as compared with from 2001 onwards (interaction p<0.0001). Before 2001, the subdistribution HR (95% CI) for cardiovascular death in patients with CML was 0.43 (0.36 to 0.52), indicating a lower risk of cardiovascular death in patients with CML as compared with controls. From 2001 onwards, the subdistribution HR (95% CI) in patients with CML was 0.99 (0.84 to 1.18), suggesting that from 2001, there was no difference in the risk of cardiovascular death between patients with CML and controls.
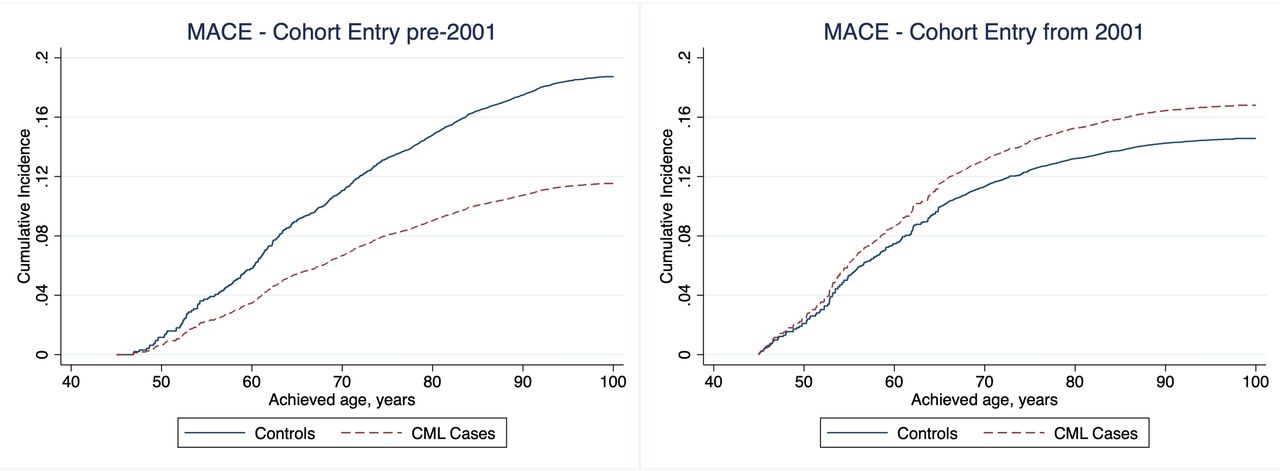
The crude MACE rate among patients with CML before 2001 was higher than among controls (table 2), although after adjustment for baseline cardiovascular risk factors, which were higher among patients with CML, the adjusted risk of MACE was lower among patients with CML than controls before 2001 (figure 1). There was a fall in MACE rates among controls from before 2001 to after 2001; however, there was no change in MACE rates among patients with CML over the same time period. The subdistribution HR for MACE differed before 2001 as compared with 2001 onwards (interaction p=0.0013). Before 2001, the subdistribution HR (95% CI) for MACE in patients with CML was 0.59 (0.46 to 0.76), indicating a lower risk of MACE among patients with CML than among controls. From 2001 onwards, the subdistribution HR (95% CI) in patients with CML was 1.27 (0.96 to 1.43).

Cumulative incidence of major adverse cardiovascular events (MACE) stratified by cohort entry before 2001 vs from 2001 and by chronic myeloid leukaemia (CML) cases versus controls, adjusted for age; sex; history of myocardial infarction, cerebrovascular disease, peripheral arterial disease, heart failure, diabetes, hypertension; chronic obstructive pulmonary disease and rural versus urban location.
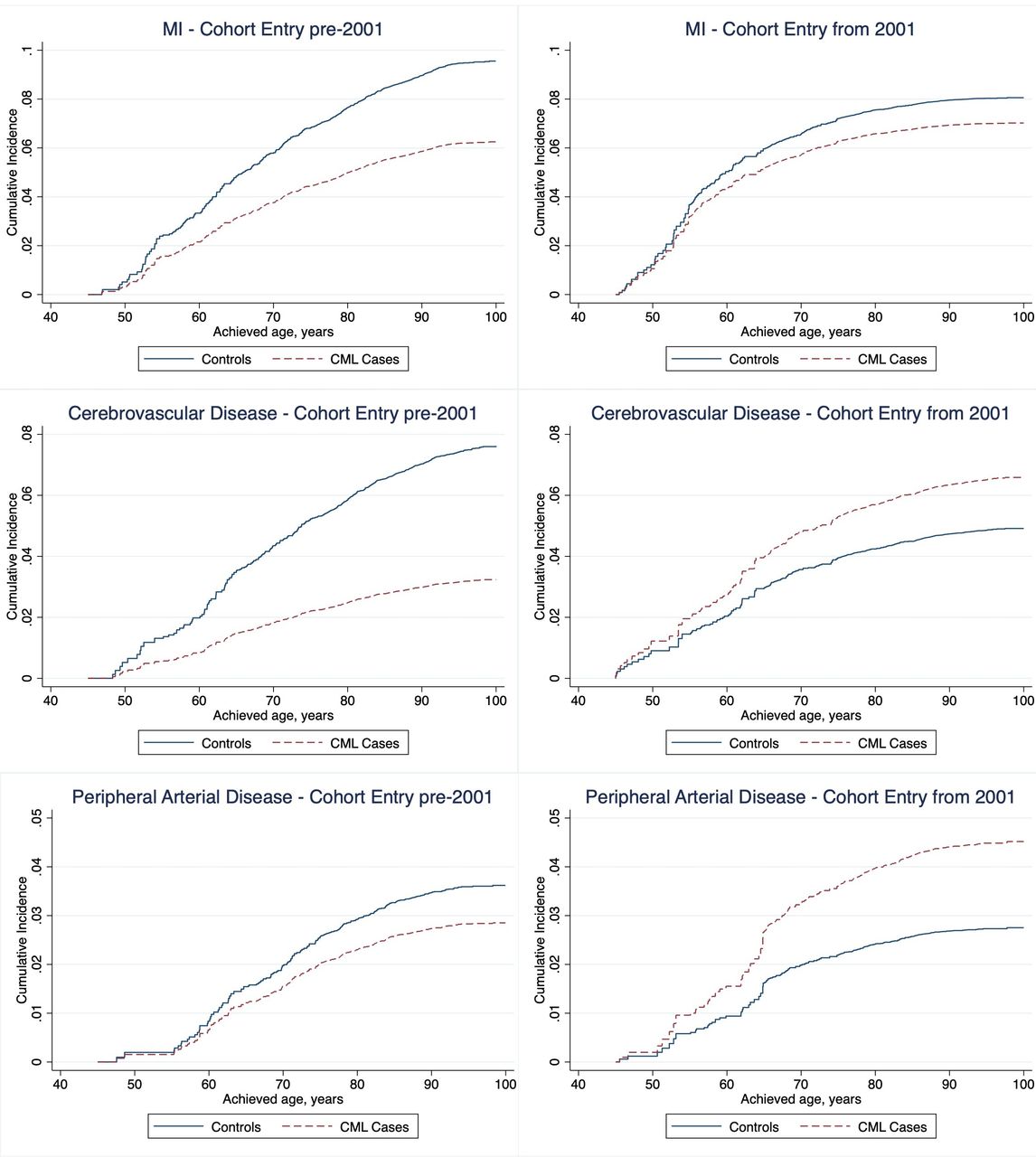
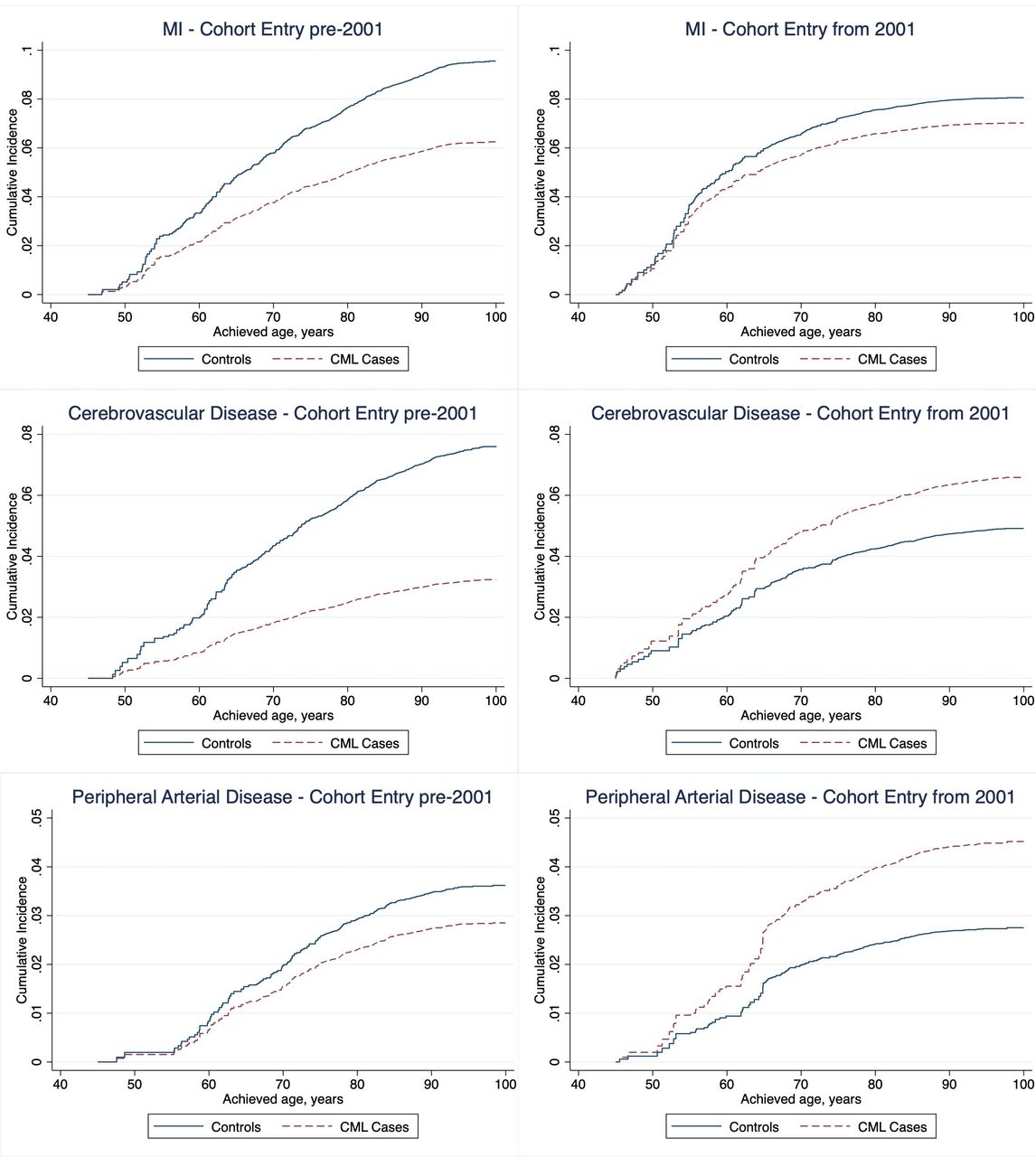
The interaction between case-control status and cohort entry pre-2001 vs from 2001 was highly significant for cerebrovascular disease (p=0.003), indicating that the risk of a cerebrovascular event differed markedly from 2001 onwards as compared with pre-2001. Before 2001, patients with CML exhibited a lower adjusted subdistribution HR of developing a cerebrovascular event (0.42 (95% CI 0.26 to 0.67)) than controls. However, from 2001 onwards, the adjusted subdistribution HR of a cerebrovascular event (1.35 (95% CI 1.00 to 1.83)) was higher among patients with CML than among controls. Similar patterns were observed for peripheral arterial disease. However, the interaction p=0.051 was not statistically significant. There was no significant interaction between year of cohort entry and the risk of myocardial infarction (interaction p=0.53). Cumulative incidence curves for outcome events in patients with CML and in controls pre-2001 and from 2001 onwards are presented in figures 1–3.

Cumulative incidence of cardiovascular death stratified by cohort entry before 2001 vs from 2001 and by chronic myeloid leukaemia (CML) cases versus controls, adjusted for age; sex; history of myocardial infarction, cerebrovascular disease, peripheral arterial disease, heart failure, diabetes, hypertension; chronic obstructive pulmonary disease and rural versus urban location.
{kind=link}
{kind=link}
{kind=link}
Cumulative incidence of myocardial infarction (MI), cerebrovascular events and peripheral arterial disease events stratified by cohort entry before 2001 vs from 2001 and by chronic myeloid leukaemia (CML) cases versus controls, adjusted for age; sex; history of MI, cerebrovascular disease, peripheral arterial disease, heart failure, diabetes, hypertension; chronic obstructive pulmonary disease and rural versus urban location.
In the sensitivity analyses, in which patients with a history of myocardial infarction, cerebrovascular disease, peripheral arterial disease or heart failure were excluded, there were no major differences to the primary analyses (online supplemental appendix table 1). In other sensitivity analyses, when MACE only included diagnostic codes that were either most responsible for length of stay, pre-admission comorbidities that contributed to length of stay or a postadmission comorbidity that contributed to length of stay, we found no significant difference from the primary analyses (online supplemental appendix table 2).
Outcomes in patients with CML according to TKI exposure
There were 1475 individuals prescribed imatinib, 486 dasatinib, 263 nilotinib, 26 bosutinib and 17 ponatinib in the database. The respective person-years of exposure to imatinib, dasatinib, nilotinib, bosutinib and ponatinib were 6710, 1137, 631, 15 and 10, respectively. We observed 158 new MACE that occurred while taking a TKI. A first MACE developed in 118 individuals while on imatinib; 20 individuals while on dasatinib; 19 individuals while on nilotinib; 1 individual while on bosutinib and no cardiovascular events were identified while on ponatinib. MACE and cardiovascular mortality rates during TKI exposure are presented in table 4. There were insufficient MACE in individuals taking bosutinib or ponatinib to estimate MACE rates on these two medications. After adjustment for cardiovascular risk factors and the duration of exposure to each individual TKI, there was no difference in the risk of a MACE while on imatinib, dasatinib and nilotinib (table 4). Compared with imatinib, the adjusted ORs (95% CI) for cardiovascular death while on dasatinib and nilotinib were respectively 0.70 (0.42 to 1.17) and 0.89 (0.50 to 1.60).
Age- and sex-standardised rates of major adverse cardiovascular events (MACE) and cardiovascular (CV) death per 1000 person-years’ drug exposure and ORs of MACE and CV death as compared with imatinib use
Discussion
Our major findings are: (1) prior to the availability of TKIs, the risk of MACE or cardiovascular death was lower among individuals with CML than controls; however, (2) since the implementation of TKIs for CML, the risk of MACE is at least as high among patients with CML as among a non-CML population and may be higher; (3) as compared with the 15-year period before 2001, the cumulative incidence of MACE among controls fell from 2001 to 2017; but little change in the cumulative incidence of MACE was seen among patients with CML over the same time; (4) we could not demonstrate a difference in the risk of MACE between imatinib, dasatinib and nilotinib in this real-world population-based cohort.
Cardiovascular risk in individuals with CML
There are few systematic data on cardiovascular outcomes in patients with CML. Prior to the TKI era, patients with CML did not survive long enough to develop MACE as outcomes were dominated by cancer progression. CML now remains the major cause of death only among patients with treatment refractory CML, a less frequent clinical state given the availability of several TKIs.
As progression-free survival has improved, patients with CML have more opportunity to develop other illnesses, such as cardiovascular disease. However, the contemporary incidence of cardiovascular events in patients with CML receiving TKIs remains unknown. In one series, cardiovascular disease accounted for only 9% of the 65 deaths reported in 559 Italian patients treated with imatinib for CML.9 In another Italian cohort of 656 patients with CML treated with second-generation or third-generation TKIs, the 15-year rate of cardiovascular death was 7%.10 In a prospective, multicentre French study of patients receiving nilotinib as first-line therapy for CML, seven (3.8%) individuals experienced an ischaemic cardiovascular event during 24 months’ follow-up.11 In a pooled analysis of 483 patients with newly diagnosed CML enrolled in clinical trials between 2000 and 2012 at a single institution, 9 (1.9%) died of cardiovascular causes.12 These findings suggest that cardiovascular outcomes were infrequent in patients with CML. The power of these studies was limited, however. In a Swedish population study, the relative risk (95% CI) of arterial events in patients with CML as compared with the general population was 1.5 (1.1 to 2.1).13 We have similarly shown that the contemporary risk (ie, since 2001) of cerebrovascular and peripheral arterial events in patients with CML is higher than among age-matched and sex-matched individuals without CML. Therefore, cardiovascular disease may be an underappreciated cause of morbidity and mortality in individuals with CML. Importantly, we found that the secular reduction in cardiovascular event rates that has been described in the general population,14 which was also seen in our control cohort, did not appear to occur among patients with CML. Consequently, those diagnosed with CML from 2001 onwards have an increased risk of cerebrovascular and peripheral arterial events than controls.
The reasons for the excess cardiovascular risk seen in patients with CML are unknown but could include unmeasured confounding factors, such as smoking quantity and duration (although we did adjust for chronic obstructive pulmonary disease) or hyperlipidaemia. In addition, we cannot exclude the possibility that CML might play a direct role in predisposing to cardiovascular disease. Clonal haematopoiesis of indeterminate potential (CHIP) has recently been recognised as a risk factor for future cardiovascular events.15 While CML is not considered CHIP, mechanisms including inflammatory cytokine release that are hypothesised to mediate the relationship between CHIP and cardiovascular events16 might also be present in CML, although this hypothesis remains to be proven. Finally, whether TKIs, as a drug class, cause MACE is unknown. TKIs are known to have off-target effects on several tyrosine kinases unrelated to CML and there are reports of varied cardiovascular adverse effects.17 Importantly, indefinite use of TKIs is the current standard-of-care for CML, so TKI cardiotoxicity is important in this population.
Cardiovascular events during exposure to different TKIs
In a systematic review of cohort studies, Chai-Adisaksopha et al evaluated the risk of arterial occlusive events associated with exposure to different TKIs.18 They found that nilotinib may be associated with a higher risk of arterial events than non-TKI-treated, imatinib-treated or dasatinib-treated patients. In our study, we did not find a significantly increased risk of cardiovascular events during nilotinib therapy as compared with imatinib. However, even with this population-based cohort, the power of our study may be limited to identify a small increase in the risk of harmful cardiovascular effects due to a specific TKI. Our findings are consistent with a more recent systematic review of 13 head-to-head randomised trials of TKIs reported by Fachi et al. 19 No difference in the risk of any serious adverse event between the different TKIs was demonstrated. However, another systematic review including 10 randomised trials found that as compared with imatinib, dasatinib, nilotinib and ponatinib were each associated with an increased risk of vascular occlusive events.2 There are possible explanations for the difference between our observational data and the randomised trial data summarised by Douxfils et al. Nilotinib or dasatinib may have been prescribed judiciously to patients in our cohort, avoiding exposure in high cardiovascular risk individuals. It is also plausible that when prescribed nilotinib or dasatinib, patients had their cardiovascular risk factors evaluated and addressed. Finally, the duration of follow-up and the cohort size in our study were limited, and longer follow-up or a larger cohort size would confer greater power to identify differences in cardiovascular event rates between the different TKIs.
Limitations
We do not have data on several cardiovascular risk factors, including smoking habits, obesity and blood cholesterol concentrations. Therefore, unmeasured confounding factors may account for the associations observed in this study. While data on patient comorbidities and cardiovascular risk factors in our study have been measured using ICD codes, such an approach is limited by inherent inaccuracies from errors in coding.20 Information on TKI prescription in Ontario is most reliably obtained for patients aged ≥65 years owing to provincial drug insurance. It is possible that patients with TKI, especially aged <65 years, in whom we have no record of TKI use, were taking TKI paid for out-of-pocket, through compassionate access schemes or private insurance. This observational study is unable to ascribe causality to the associations observed. Outcome events in the CML cohort were ascribed to the TKI they were dispensed last. We cannot exclude the possibility that previous CML therapies contributed to the occurrence of the event of interest. We did not have enough patient-years exposure to ponatinib or bosutinib to evaluate their associations with adverse cardiovascular events.
Conclusions
Patients with CML in the era of TKI use are at increased risk of adverse cardiovascular outcomes as compared with adults from the general population. Further research is needed to evaluate the importance of strategies to reduce cardiovascular risk in patients with CML and in particular to mitigate the increased cardiovascular risk conferred by some newer TKIs.
Key messages
What is already known on this subject?
It is known that tyrosine kinase inhibitors are highly effective long-term treatments for chronic myeloid leukaemia (CML), but that they can cause serious adverse cardiovascular events.
What might this study add?
The improvement in CML survival that has resulted from the widespread use of tyrosine kinase inhibitors has changed the spectrum of clinical outcomes that can adversely affect patients with CML.
In a contemporary population of patients with CML, the risk of some adverse cardiovascular outcomes may now exceed the risk seen in a non-CML patient population of similar age and sex distributions.
How might this impact on clinical practice?
Cardio-oncology programmes are increasing in number.
Our findings affirm the importance of such programmes to address the contemporary needs of individuals with CML.
Acknowledgments
The authors would like to thank IQVIA Solutions Canada Inc. for use of their Drug Information Database and Cancer Care Ontario for use of their Ontario Cancer Registry.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DarrylLeong
Contributors DL designed the study, conducted analyses, drafted the manuscript and is responsible for the overall content as guarantor. NA, CH, DS, SK, SR, GP and HS contributed to the interpretation of the analyses and edited the manuscript. HS facilitated access to the data. The corresponding author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence (or non-exclusive for government employees) on a worldwide basis to the BMJ Publishing Group Ltd (BMJPGL) and its Licensees to permit this article (if accepted) to be published in HEART editions and any other BMJPGL products to exploit all subsidiary rights.
Funding Funding was provided by the Population Health Research Institute, McMaster University. DL has received support from the Canadian Institutes of Health Research, the Heart and Stroke Foundation of Canada, the Canadian Cancer Society and the Cancer Research Society. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). ICES is an independent, non-profit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyse healthcare and demographic data, without consent, for health system evaluation and improvement. Parts of this report are based on Ontario Registrar General information on deaths, the original source of which is ServiceOntario.
Disclaimer The opinions, results and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval This study was conducted in accordance with the Declaration of Helsinki and was approved by the Hamilton Integrated Research Ethics Board, Canada. The public was not involved in the design or execution of the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. Raw data are available on successful application to the Institute of Clinical and Evaluative Sciences, Ontario, Canada.