Article Text

Abstract
Clinical introduction A 45-year-old man with ulcerative colitis was admitted with bloody diarrhoea and chest pain. Inflammatory markers and high-sensitivity troponin were elevated (C reactive protein 57 mg/L, white cell count 10.65×109/L, neutrophil 6.6×109/L, Troponin-I 663 mmol/L). The ECG showed inferior ST-elevation. Urgent coronary angiography revealed unobstructed coronary arteries. Inpatient cardiovascular magnetic resonance (CMR) was arranged to determine the aetiology of the myocardial infarction with non-obstructive coronary arteries. The imaging protocol at 1.5 T included balanced steady-state free precession cine images, T2-weighted oedema sequences, and early and late gadolinium enhancement (LGE). Native T1 and T2 mapping images provided advanced tissue characterisation (figure 1).
Question What is the most likely diagnosis based on the MRI findings?
Multiple embolic myocardial infarctions in the right coronary artery territory.
Acute autoimmune myocarditis.
Cardiac sarcoidosis.
Stress (Takotsubo) cardiomyopathy.
Multiple embolic myocardial infarctions in the left circumflex coronary artery territory.

{kind=link}
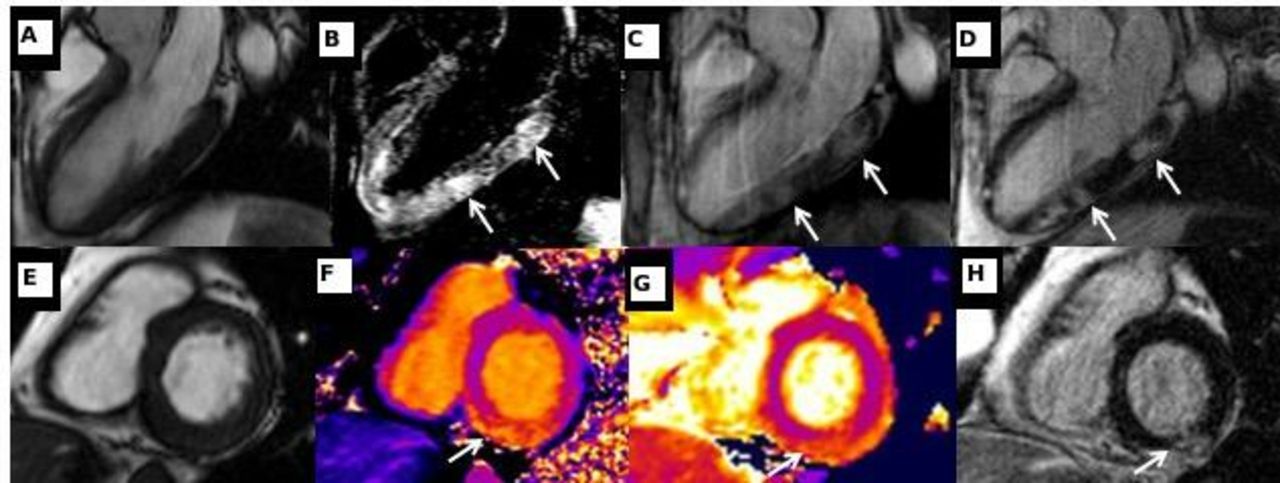
(A) Balanced steady-state free precession (bSSFP) left ventricular long-axis, three-chamber view. (B) T2 short-tau inversion recovery. (C) Early gadolinium enhancement demonstrating high signal intensity indicative of hyperaemia with capillary leakage (arrowed). (D) Late gadolinium enhancement with high signal intensity indicative of increased extracellular space (arrowed). (E) bSSFP left ventricular short-axis view. (F) Native myocardial T1 mapping with elevated native T1 mapping values in the inferior wall (arrowed). (G) Native myocardial T2 mapping with elevated native T2 values in the inferior wall, indicative of oedema (arrowed). (H) Late gadolinium enhancement with high signal intensity indicative of increased extracellular space (arrowed).
- cardiac magnetic resonance (cmr) imaging
- acute coronary syndromes
- myocarditis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Answer B
Multiple patchy, mid-myocardial, high-intensity signal areas in the inferolateral wall on T2-weighted images (B) and increased T2 mapping values on the short-axis images (G) are highly specific for oedema. These areas have high signal intensity on early (C) and late (D,H) sequences, suggesting hyperaemia with capillary leakage and increased extracellular space, respectively. Furthermore, increased native T1 mapping values in all layers but predominantly in the subepicardium of the entire lateral wall (F) are in keeping with extensive myocardial injury (figure 1). Taken in combination, these findings meet the updated Lake Louise criteria for acute myocarditis.1 Despite extensive oedema, stress (Takotsubo) cardiomyopathy (option D) can be excluded by ventricular morphology and the presence of LGE,2 and multiple embolic myocardial infarctions (options A and E) are excluded by the non-ischaemic pattern of LGE.3 Finally, based on the CMR, cardiac sarcoidosis (option C) cannot be easily distinguished from acute autoimmune myocarditis. However, the clinical presentation and absence of pulmonary changes make the latter diagnosis the most likely.4 Cardiac biopsy might definitively differentiate, but is not routinely performed due to associated procedural risk. The patient was treated with corticosteroids and monoclonal antibodies and responded well. The pathophysiological mechanisms underlying cardiac manifestations of inflammatory bowel disease are incompletely understood but may occur in up to one-third of patients with inflammatory bowel disease.5
Acknowledgments
BB identified and reported the case, conceived the idea of publication as a case report, and wrote and revised the manuscript. IH obtained informed consent, helped write the manuscript and revised it critically for important intellectual content. CB-D reported the clinical case, jointly conceived the idea of a case report and revised the manuscript critically for important intellectual content.
Footnotes
Funding CB-D is in part supported by the NIHR Biomedical Research Centre at the University Hospitals Bristol NHS Foundation Trust and the University of Bristol.
Disclaimer The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, or the Department of Health and Social Care.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.