Article Text

Abstract
Situs inversus with dextrocardia occurs in approximately one in 10 000 patients. Successful stent deployment for the treatment of unstable angina and situs inversus is presented. Three technical challenges associated with the procedure are highlighted. Firstly, the successful choice of diagnostic and interventional catheters is based on an understanding of the orientation of the aortic arch. With a right sided aorta Judkins catheters should be successful. Secondly, image reversal is not necessarily required for image interpretation. Thirdly, successful coronary engagement with catheters requires rotation in a direction opposite to that normally used.
- dextrocardia
- situs inversus
- stenting
- unstable angina
Statistics from Altmetric.com
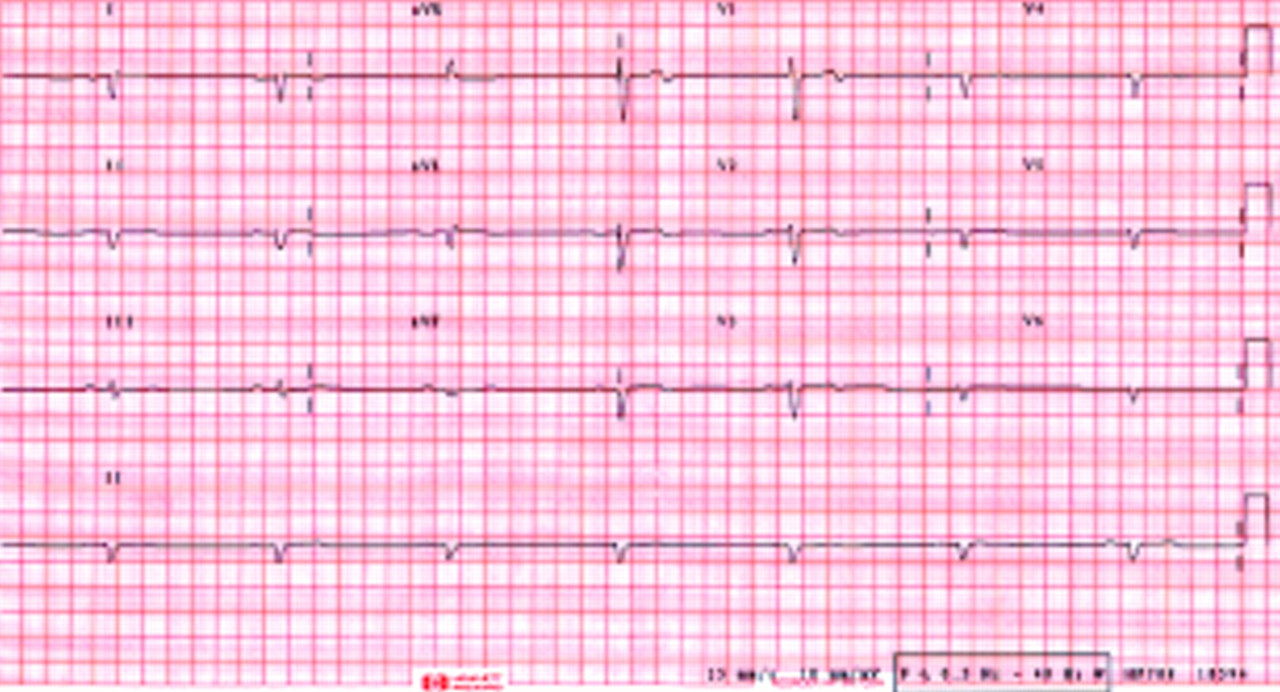
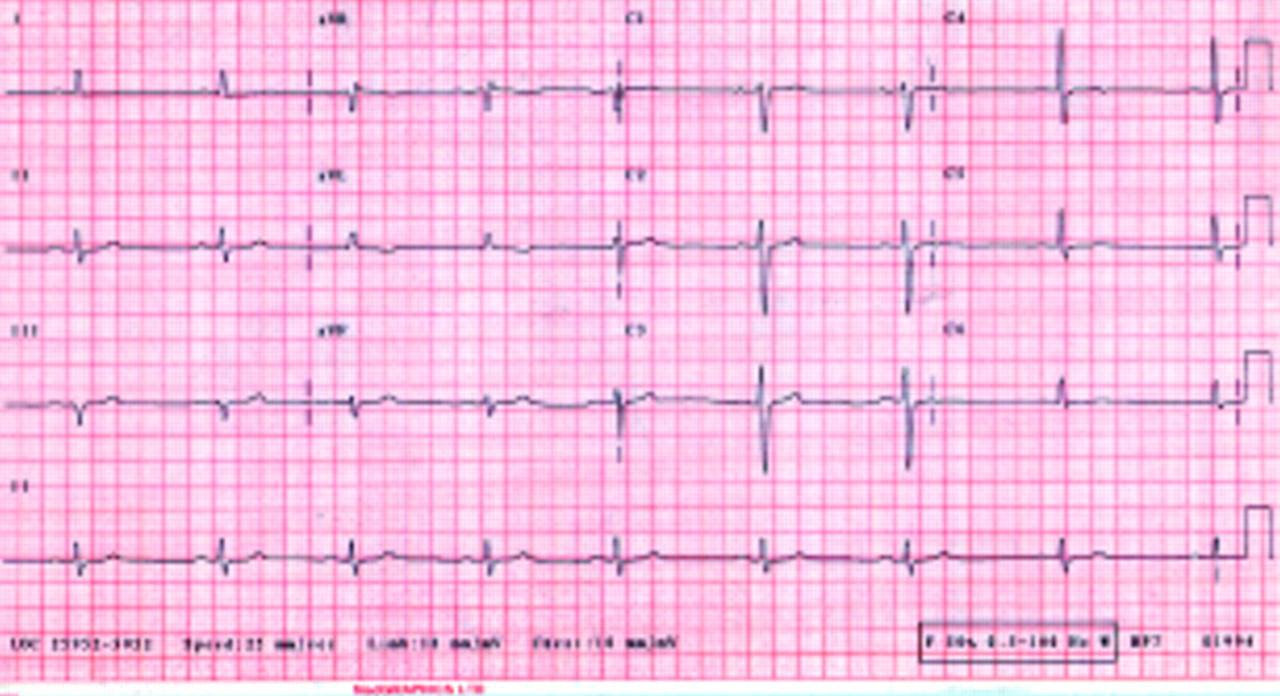
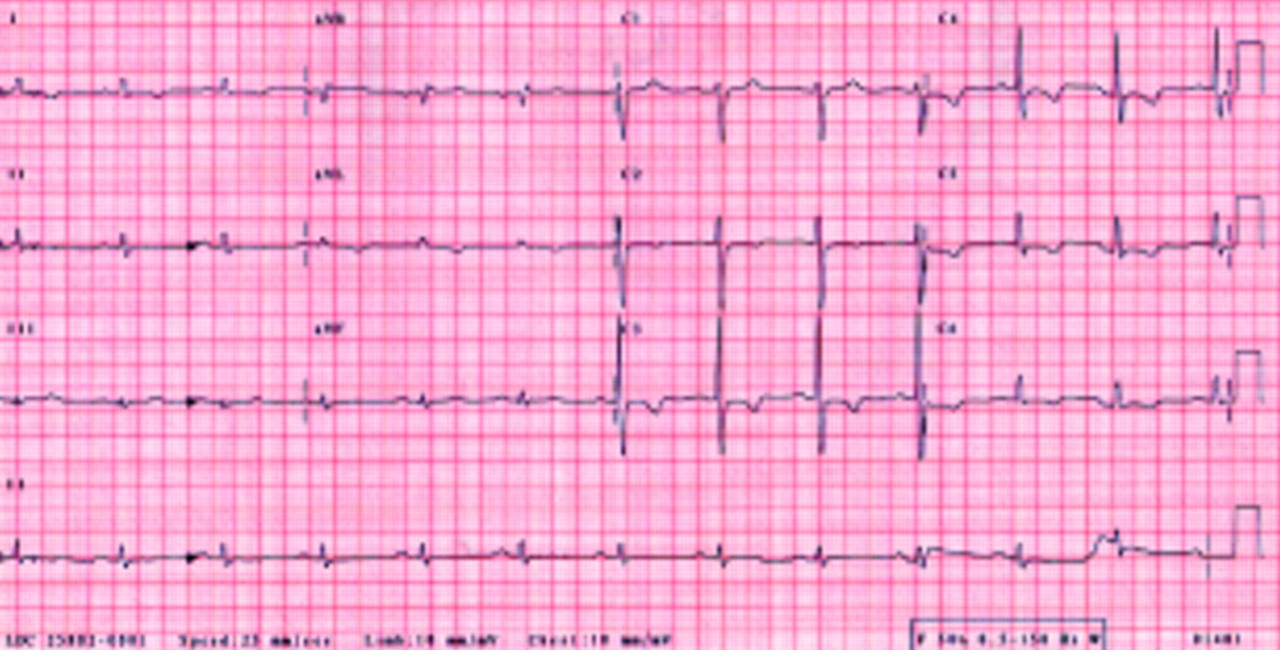
A 66 year old man presented with chest pain at rest. He had suffered for the previous two years angina on exertion. Clinical examination showed a right sided apex beat. The liver was left sided and the spleen right sided. The admission left sided ECG showed a reduction in the R wave voltage across the chest leads (fig 1) in contrast to the right sided ECG (fig 2). In chest pain the right sided leads showed flattening of the ST segments and deepening of the T wave inversion (fig 3). Risk factors for ischaemic heart disease included hypercholesterolaemia, hypertension, and a positive family history. His medical history included documented situs inversus, sinusitis, and bronchiectasis. Initial management of his acute coronary syndrome was with aspirin, low molecular weight heparin, and intravenous nitrate. Subsequent peak creatine kinase was 260 IU/l.

Left sided ECG while the patient was pain free.

Right sided ECG while the patient was pain free.

Right sided ECG during chest pain.
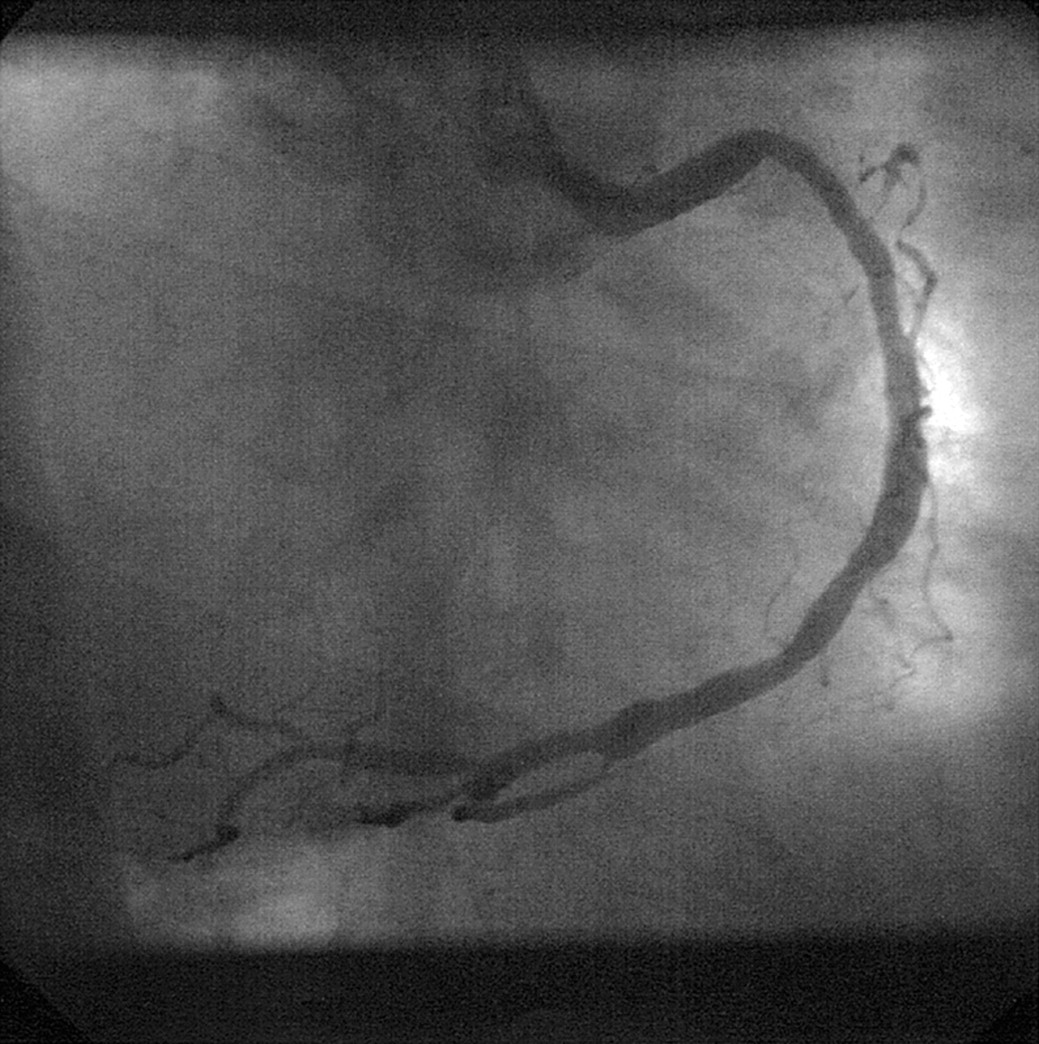
Coronary angiography was performed from the right femoral artery. The anatomical right coronary (left sided) was cannulated with a right Judkins 4 catheter and was found to be atheromatous but without a critical lesion (fig 4). The anatomical left coronary system (right sided) was cannulated with a left Judkins 5 catheter. The left anterior descending artery was again only atheromatous but the circumflex artery had a proximal critical stenosis (fig 5). Left ventricular function was good (fig 6).

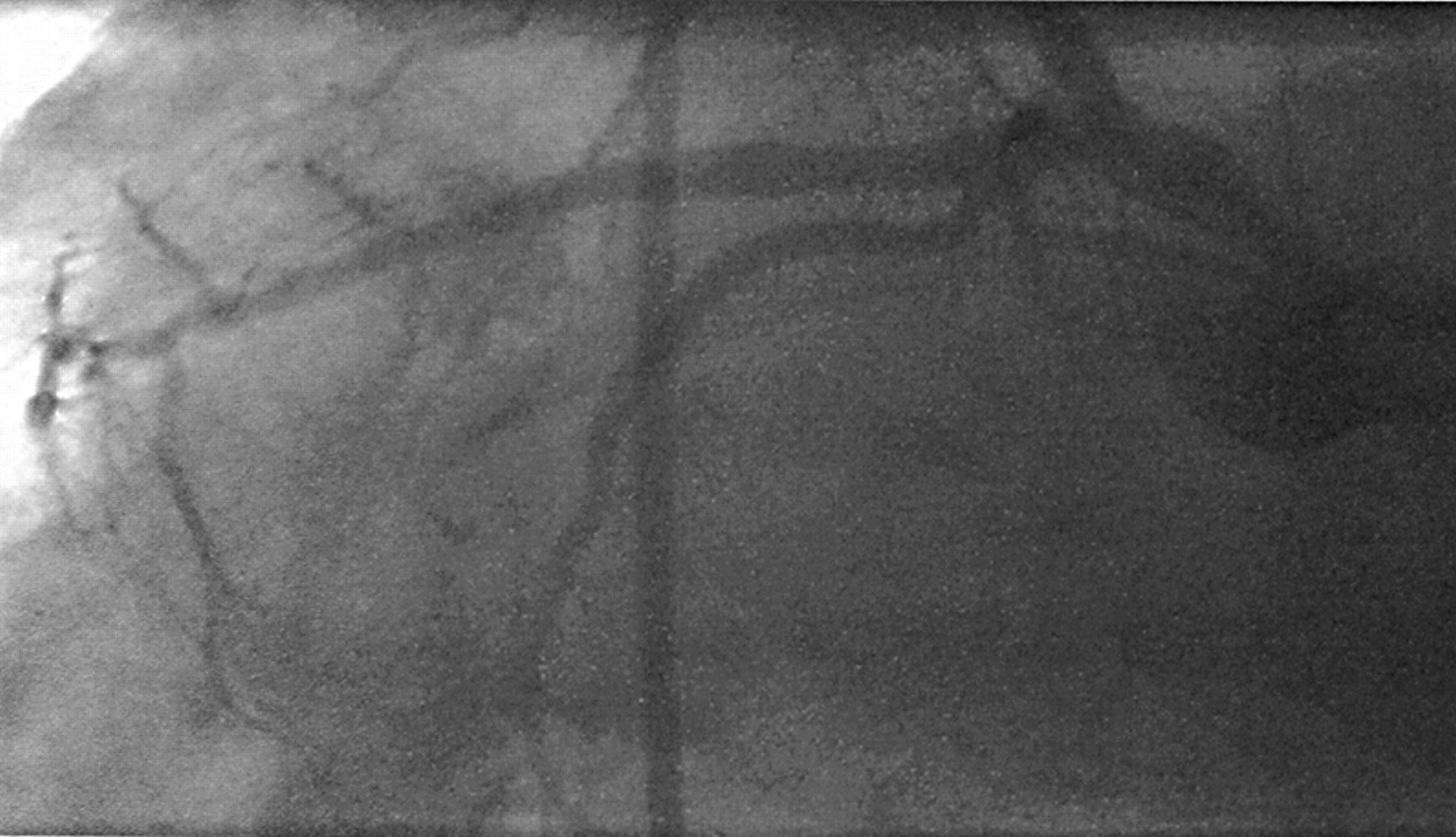
Right anterior oblique (RAO) coronary angiogram of left sided right coronary artery.

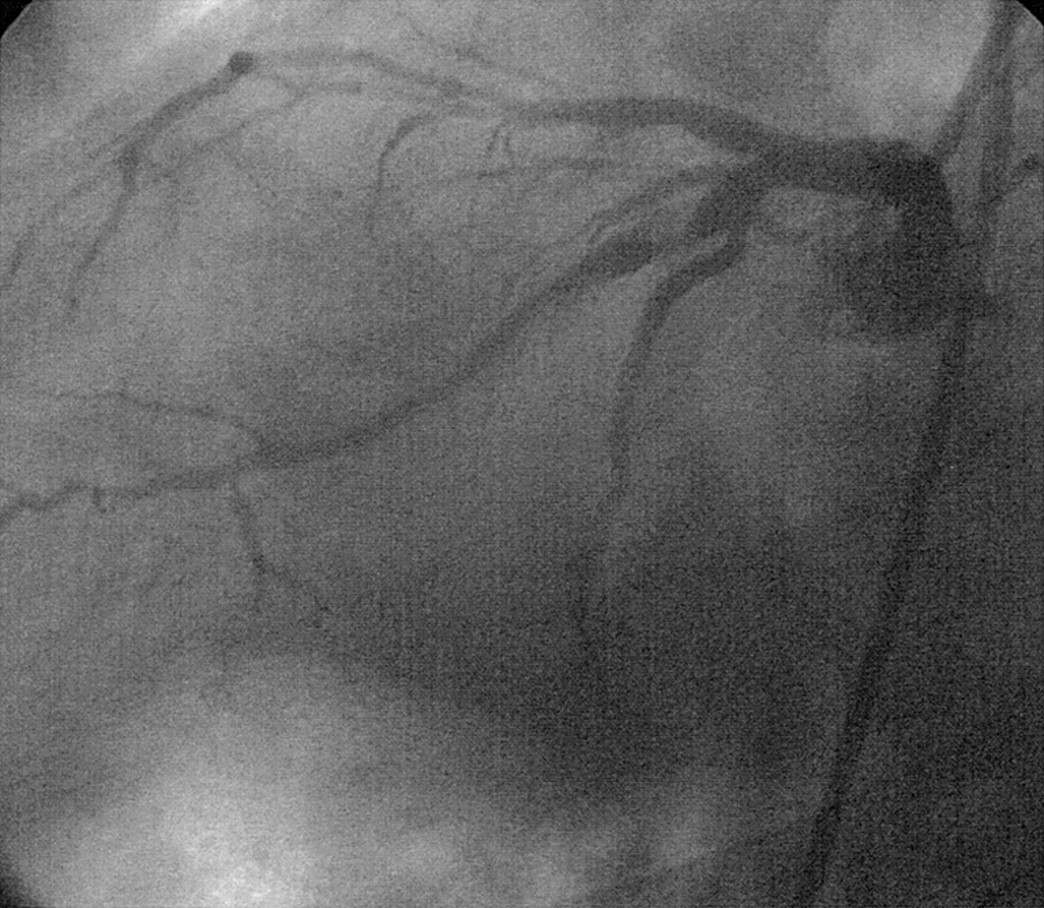
Left anterior oblique (LAO) caudal coronary angiogram of right sided left coronary artery.

LAO left ventriculogram.
In view of the unstable presentation and ongoing chest pain, angioplasty and stent insertion were performed the following day. An 8 French left Judkins 5 guide catheter was used to cannulate the right sided left coronary system. The critical lesion was visualised in the right anterior oblique caudal (fig 7, spider) and the left anterior oblique caudal (fig 8) views. The procedure was performed without reversing the right to left presentation of the images. The lesion was crossed with a 0.014 inch high torque floppy wire and predilated with a 3.0 mm monorail balloon. The lesion site was then stented with a 3.5 mm by 18 mm Duet stent (Guidant, Santa Clara, California) deployed to 16 atm. In view of significant distal disease evident after stent deployment the first stent was overlapped distally with a 3.0 mm by 18 mm Duet stent deployed to 16 atm producing a satisfactory angiographic result (fig 9). Following the procedure the patient was treated with aspirin and four weeks' clopidogrel. The patient remained asymptomatic at six months' follow up.

RAO caudal view of circumflex stenosis before stent deployment.

LAO caudal view of circumflex stenosis before stent deployment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
RAO caudal view of final result after stent deployment.
Discussion
Situs inversus with dextrocardia occurs in approximately one in 10 000 patients.1 Of these patients 15% have Kartagener's syndrome (immotile cilia syndrome), which affects approximately one in 68 000 and is inherited as an autosomal recessive trait.2 The association of coronary heart disease is at the same frequency as in the general population.3 In the management of situs inversus the first cardiac catheterisation was performed in 1973,4 the first coronary bypass surgery in 1980,5 and the first percutaneous transluminal coronary angioplasty in 1987.6
To our best knowledge, since 1987 there have been 12 reports of the percutaneous treatment of coronary stenoses in dextrocardia.7-9 This case report documents successful stent deployment for the treatment of a coronary stenosis in dextrocardia. The objective of this report is to highlight three technical challenges associated with the procedure. Firstly, our experience was that the choice of diagnostic and interventional guide catheters that provided adequate access to the coronaries and support for stent deployment could be predicted by the position of the aorta. Thus, in our case with a right sided aortic arch the right sided left coronary artery could be successfully cannulated with a left Judkins catheter manipulated to a mirror image of its normal position. Conversely the left sided right coronary was cannulated with a right Judkins catheter again manipulated to a mirror image of its normal position (fig 4). It was our experience that the left Judkins guide catheter provided adequate support for stent deployment with the use of a high torque floppy wire alone. This approach of using Judkins catheters positioned in the mirror image has found support from other operators,10 although following the first ever procedure Moreyra and colleagues6 stated that the Judkins catheters were unhelpful and suggested the use of a multipurpose catheter or a brachial approach. Secondly, it was our experience that angiography and intervention could be performed by using standard image acquisition. Although it is possible to select right to left image reversal throughout, we did not find it necessary to do so. For intervention to the circumflex artery we simply worked in the right anterior oblique caudal projection (fig 7) producing an image recognisable as a mirror image “spider view” and the normal left anterior oblique caudal projection (fig 8), which produced an image recognisable as a mirror image of the normal right anterior oblique caudal. Thirdly, successful rotation of the catheters was in the opposite direction. Thus, for the left sided right coronary artery, engagement with the right Judkins catheter required anticlockwise rotation.
In summary we report an extremely rare case of the percutaneous treatment of a coronary stenosis in situs inversus. The use of Judkins catheters, standard image acquisition, and counter rotation of catheters allowed the stenting procedure to be uncomplicated.